

Central vascular access plays a key role in the administration of vesicant and/or long-term intravascular therapies. However, the insertion of a central venous catheter may involve risks such as infection, thrombosis, or accidental catheter dislodgement. For this reason, subcutaneous tunneling has become an increasingly used technique to minimize these risks and improve patients’ quality of life.
In this article, we review what the RAVESTO tool proposes and how it can be of great help in patients with particularly difficult vascular access.
Summary
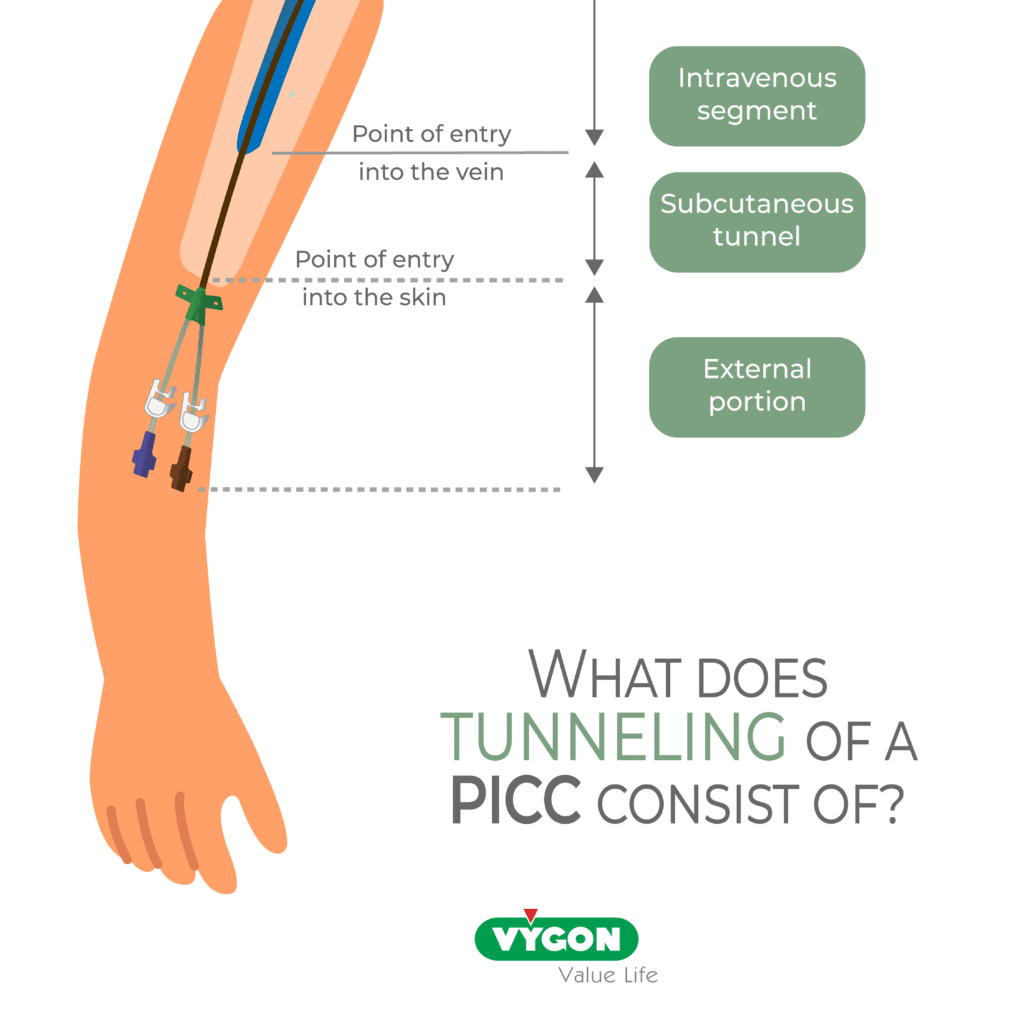
- Subcutaneous tunneling consists of cannulating a vein and selecting a catheter exit site that is different from the venous entry point, creating a tunnel between the venous insertion site and the skin exit site.
- In patients with very complex vascular access and/or cognitive impairment, it is often necessary to use different tunneling techniques in order to choose the one that best adapts to the patient’s needs. Among other factors, it is important to assess the presence of tracheostomy, skin lesions, areas prone to infection.
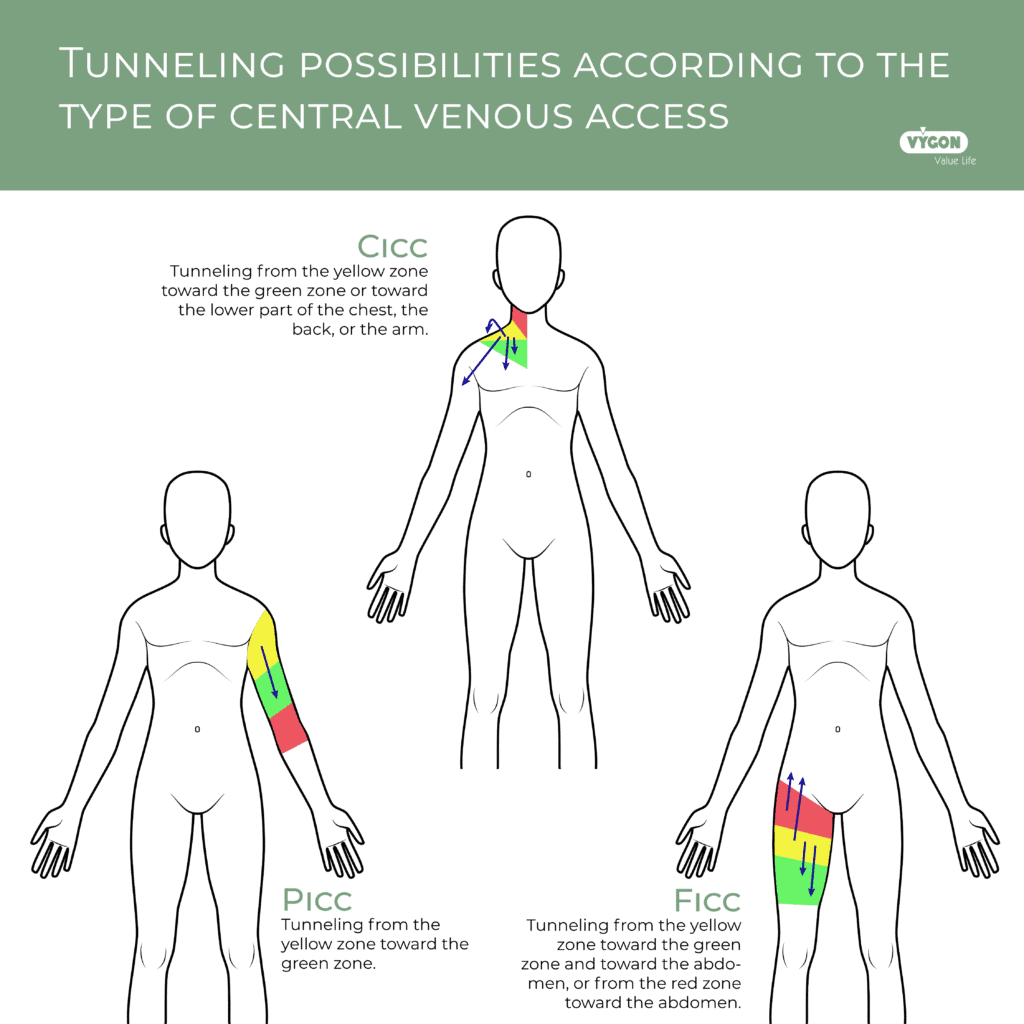
- In the case of PICC lines, tunneling is usually performed from the yellow zone to the green zone, whereas with CICC and FICC, it is possible to create longer tunnels that go beyond the areas defined by the ZIM method, ensuring better fixation and a lower risk of infection (respectively in the arm or back, and in the abdomen).
What Does Tunneling of a Vascular Access Consist Of?
Tunneling consists in the creation of a subcutaneous tunnel between the catheter insertion site into the vein and the catheter exit site at the skin level. This technique allows greater catheter stability and a reduction in the risk of infection.
Why Does It Minimize the Risk of Catheter Dislodgement?
When a tunnel is created beneath the skin, subcutaneous tissues gradually adhere to the device, generating firmer fixation.
In addition, if traction is exerted on the catheter extension, the force is applied to the subcutaneous portion rather than directly at the venous entry site, significantly reducing the risk of accidental removal.
Why Does It Reduce the Risk of Infection?
By increasing the distance between the skin exit point and the venous insertion site, the subcutaneous segment of the catheter acts as a natural antimicrobial barrier, reducing the risk of microorganism migration toward the bloodstream.
Why Use Tunneling?
When assessing a patient’s veins, it may occur that a vein with an adequate diameter is not located in the ideal puncture area defined by the ZIM method (green zone). In this context, veins located in the yellow zone may need to be considered. To ensure that the catheter exit site remains in the safer green zone, the device can be tunneled.
In this way, the external portion of the catheter remains away from areas more prone to infection, such as the axilla, the groin and the oral area.
With improvements in care and in overall health, patients live longer. However, this leads to repeated hospitalizations and progressively, to the deterioration of their venous capital. This context complicates the options available to healthcare professionals to access veins. In addition, certain groups of elderly patients present cognitive impairment, which makes their cooperation difficult and represents a high risk of catheter removal.
What is RAVESTO?
Definition
RAVESTO is the Rapid Assessment of Vascular Exit Site and Tunneling Options in vascular access.
Its purpose is to define the different subcutaneous tunneling options and their indications in different clinical situations in patients with complex vascular access.
As the authors of the RAVESTO method remind us, for decades, tunneling was considered only for cuffed catheters and fully implanted devices, such as, Hickman catheters and chest ports.
However, in recent years, bedside tunneling of non‑cuffed central venous access devices has also gained acceptance. The choice of the catheter exit site is crucial to minimize the risks associated with catheter insertion.
The tool consists of three main parts:
- Exit‑site assessment: This section evaluates the characteristics of the exit site, such as skin type, depth, and location. Factors such as the presence of scars and the accessibility of the site for both the patient and the healthcare professional are also considered.
- Vein assessment: This section evaluates the patient’s vein, including vein quality, size, location, and depth. Factors such as the presence of obstructions and the accessibility of the vein for the healthcare professional are considered.
- Assessment of the need for tunnels: This section evaluates the need for tunneling based on the location of the exit site and the patient’s vein. Factors such as the length of the vascular access, the need to avoid obstructions, and the need to reduce the risk of infection are considered.
Selection of the catheter exit site
The exit site should be chosen based on areas with a higher risk of contamination and/or according to the risk of displacement, especially in patients with cognitive impairment.
The choice of the exit site may also depend on:
- the duration of the therapy,
- the previous device history,
- the patient’s underlying comorbidities.
What material should be used for tunneling?
Tunneling can be performed using a dedicated tunneling device (tunneler), either metal or plastic, but also by using a short peripheral catheter. In this case, since the tunneling is very short, it is referred to as “pseudo‑tunneling.”
In general, it consists of two fundamental steps (anterograde tunneling):
- Venous puncture under ultrasound guidance followed by placement of a guidewire for cannulation
- Subcutaneous tunneling to introduce the catheter from the exit site toward the puncture site
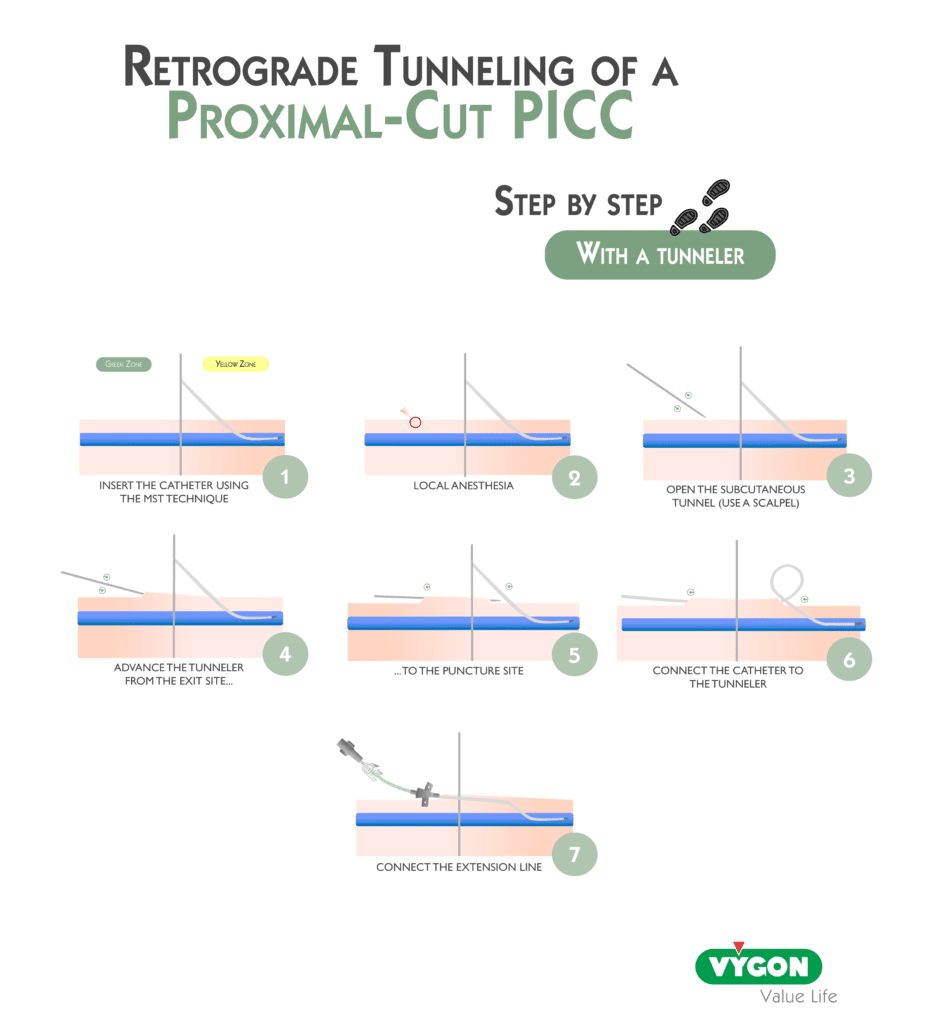
In the case of catheters with a proximal cut, retrograde tunneling is performed: the catheter is passed from the puncture site toward the exit site.
When should the RAVESTO protocol be used and why?
Type of central vascular access devices that can be used with RAVESTO
RAVESTO is a tool intended for the placement of devices with an external portion. It is a protocol applicable to the insertion of PICC, CICC, and FICC.
PICC
As mentioned previously, in order to access a vein of larger caliber while keeping the catheter exit site in the appropriate zone, tunneling can be performed from the yellow zone to the green zone.
CICC
In the case of a central catheter, from the puncture site when the approach is supraclavicular, tunneling can be directed toward:
- the infraclavicular area (for example, in the case of tracheostomy),
- the arm (when there is not an adequate skin condition on the thorax),
- the back (in disoriented patients).
When the approach is infraclavicular, tunneling can be performed as follows:
- the infraclavicular area (for example, in the case of tracheostomy),
- the arm (when there is not an adequate skin condition on the thorax),
- the back (in disoriented patients).
FICC
It is preferable to cannulate this type of vascular access in the superficial femoral vein, since according to recommendations, a femoral central catheter inserted in the common femoral vein must be removed after 48 hours due to the increased risk of infection associated with its proximity to the groin area.
In this case, it is possible to tunnel the catheter:
- toward the mid‑thigh,
- toward the distal third of the thigh (to better prevent the risk of infection and accidental dislodgement),
- toward the abdomen (for the same reason).
Why use the RAVESTO protocol in daily practice?
When facing patients with complex or very complex vascular access, it is necessary to have a guide that offers the best possible recommendations for the cannulation of a central vascular access.
When this resource cannot be used or has not been considered, the probability of vascular access failure increases and, as a result, the patient may experience catheter displacement or accidental removal.
If the catheter has lost its central position, there is a risk of:
- Thrombosis
- Malfunction
- Endothelial damage
- Incorrect measurement of central venous pressure (CVP)
If the catheter has been removed, this entails:
- A delay in intravenous treatment
- Re‑insertion of a catheter, which can be complex in DIVA patients
It is important to carry out a rigorous evaluation that considers the risks and benefits associated with the selection of the exit site and the placement of recommended tunnels. This information is vital so that healthcare professionals can make appropriate decisions regarding patient care and the management of vascular access.
Once applied, the RAVESTO protocol provides:
- valuable and detailed information about the patient’s vascular access
- clear recommendations that take into account the risks related to the exit site and tunnel placement for the patient
Associated with a global analysis of the patient (medical history, habits), the type of drugs to be infused and their duration, as well as the appropriate choice of catheter, this method makes it possible to maximize the probability of vascular access success for the required period of time.
It should be taken into account that exit‑site selection and tunnel placement are crucial factors in the management of patients with complex vascular access.
The exit site must be carefully evaluated to minimize the possibility of infection, extravasation, and thrombosis, while tunnel creation must be appropriate to ensure adequate blood flow and reduce the risk of complications.
Tunneling can improve patient comfort and reduce the risk of accidental catheter removal in patients with cognitive impairment.
Bibliography
- Matt Ostroff, Philippe Moureau y Mauro Pittiruti, Rapid Assessment of Vascular Exit Site and Tunneling Options (RAVESTO): A new decision tool in the management of the complex vascular access patients, journal of vascular access, 24(2):311-317, Marzo – 2023
- Robert Dawson PICC Zone Insertion MethodTM (ZIMTM): A Systematic Approach to Determine the Ideal Insertion Site for PICCs in the Upper Arm, JAVA Vol 16 No 3 – 2011
- Emoli et al., The ISP (Safe Insertion of PICCs) protocol: a bundle of 8 recommendations to minimize the complications related to the peripherally inserted central venous catheters (PICC), Assist Inferm Ric ; 33(2): 82–89, april-june – 2014
- Brescia et al. Rapid Femoral Vein Assessment (RaFeVA): a systematic protocol for ultrasound evaluation of the veins of the lower limb, so to optimize the insertion of femorally inserted central catheters; 22(6):863-872, November 2021.
- Pittiruti y Scoppettuolo, Manual GAVeCeLT sobre PICC y midline – 2016
- INS Guidelines 2021




