Radial arterial catheters are foundational to hemodynamic monitoring and blood sampling across anesthesia, intensive care, and emergency medicine. Yet preventable complications—mechanical instability after wrist flexion, catheter kinking due to steep insertion angles, site infection, and premature line failure—remain common.
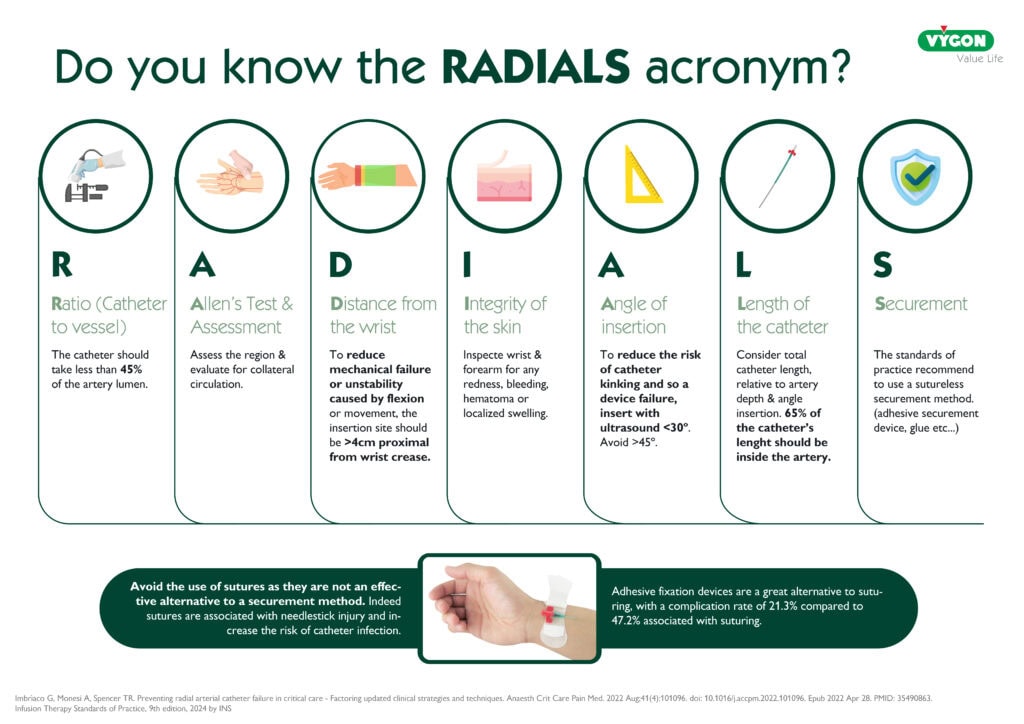
This article synthesizes the RADIALS2 framework (Ratio, Allen’s test & Assessment, Distance from the wrist, Integrity of the skin, Angle of insertion, Length of catheter, Securement) into a cohesive, academically styled guide for insertion and maintenance.
Despite their ubiquity, radial arterial lines fail more often than they should. Many failures trace back to a handful of modifiable factors: selecting an oversized catheter relative to the artery, cannulating too close to the wrist crease, accepting compromised skin, entering at a steep angle that predisposes to kinking, advancing too little of the catheter into the lumen, and relying on sutures for securement. Clinicians often know pieces of this puzzle; the challenge is executing them reliably and together—especially when cognitive load is high.
The RADIALS framework was developed to make these priorities memorable and actionable, distilling best practice into seven linked decisions that influence both insertion success and ongoing performance.
THE RADIALS FRAMEWORK
RATIO (R): CATHETER‑TO‑ARTERY PROPORTION
Select a catheter whose external diameter is less than 45% of the arterial lumen. Respecting the vessel’s caliber reduces endothelial trauma and the risk of occlusion, while preserving downstream perfusion. Ultrasound sizing supports this decision by providing a real‑time estimate of luminal diameter.
ALLEN’S TEST & ASSESSMENT (A): PERFUSION FIRST
Before puncture, verify collateral circulation (e.g., with Allen’s test or equivalent) and assess the region for anatomic suitability. This step is a perfusion safeguard and a contextual check: vascular variants, prior interventions, or localized edema can complicate cannulation or compromise safety if overlooked.
DISTANCE FROM THE WRIST (D): BUFFER AGAINST FLEXION
Cannulate more than 4 cm proximal to the wrist crease. This spatial buffer reduces the lever‑arm forces generated by everyday movements—transport, imaging, patient repositioning—that otherwise destabilize catheters and degrade waveforms. Flexion‑related mechanical failure is less likely when the entry site is not at the hinge point of motion.
INTEGRITY OF THE SKIN (I): INFECTION PREVENTION AT THE SOURCE
Avoid insertion through tissue with redness, bleeding, hematoma, swelling, burns, or lesions. Compromised skin increases microbial burden, weakens dressing adherence, and raises the risk of local infection. Selecting intact skin is therefore a primary prevention step, not an aesthetic preference.
ANGLE OF INSERTION (A): GEOMETRY AGAINST KINKING
Under ultrasound guidance, maintain an entry angle below 30° and avoid angles over 45°. Shallow angles smooth the catheter’s path into the lumen and lower the probability of kinking—one of the most frequent contributors to damped or intermittent waveforms and premature device failure.
LENGTH OF THE CATHETER (L): INTRALUMINAL STABILITY
Advance so that approximately 65% of the catheter’s length resides within the artery. Too little length invites instability and dislodgement; too much may complicate care without added benefit. The ~two‑thirds target balances stability with functional transduction and ease of maintenance.
SECUREMENT (S): SUTURE‑FREE BY DESIGN
Use an adhesive securement device, an integrated securement system, a subcutaneous anchor, or tissue adhesive, always in addition to a primary dressing. Avoid sutures, which are associated with needlestick injury and higher infection risk; in the data cited, overall complications with suturing were 47.2%, compared with 21.3% for adhesive fixation1. Opting for suture‑free strategies therefore advances both staff safety and patient outcomes.
PRACTICAL APPLICATION
Applying RADIALS is less about linear steps than about maintaining a coherent mental model throughout the procedure. Pre‑procedure ultrasound supports both Ratio and Distance decisions, while visual and tactile inspection address Integrity. During cannulation, real‑time ultrasound helps maintain the recommended Angle and verify intraluminal placement to achieve the target Length. Immediately post‑insertion, attention turns to Securement—choosing a non‑suture approach that stabilizes the device without increasing sharps exposure or undermining dressing performance. This framing extends seamlessly into maintenance: daily assessments revisit skin integrity, dressing condition, and line stability with the same intentionality as the original insertion.
RISK MITIGATION AND TROUBLESHOOTING
A small set of recurring problems accounts for most unplanned line interventions, and RADIALS aligns directly with their prevention:
- Flexion‑related instability often reflects distal site selection. Reconsider Distance if waveforms degrade after patient movement.
- Kinking or intermittent tracing is commonly geometric. Reassess Angle (aim for <30°) and confirm the catheter’s course under ultrasound.
- Local infection or dressing failure usually traces back to Integrity and Securement. Prioritize intact skin and suture‑free stabilization to minimize microbial load and handling.
- Perfusion concerns call for revisiting Ratio and Allen’s test, ensuring lumen‑sparing device choice and collateral flow were confirmed.
- Early dislodgement suggests insufficient Length in the lumen or suboptimal securement; adjust both to restore stability.
CONCLUSION
RADIALS consolidates the decisions that most determine the success and safety of radial arterial catheterization into a compact, reproducible framework. By integrating vessel respect, perfusion safeguards, movement‑aware site selection, geometry‑conscious insertion, evidence‑aligned intraluminal length, and suture‑free securement, teams can reduce preventable complications and improve line performance. The value of RADIALS lies not only in its individual elements but in how it helps clinicians enact them consistently—especially when the stakes and cognitive demands are highest.
REFERENCES
- Infusion Therapy Standards of Practice, 9th edition, 2024 by INS
- Imbriaco G, Spencer TR, Bardin-Spencer A. 10 best practice tips with radial arterial catheterization. The Journal of Vascular Access. 2022;25(2):363-368. doi:10.1177/11297298221101243
A place to learn about health procedures and techniques from leading professionals.




