
The midline catheter growth has been exponential since it is a resource that allows a notable improvement in the management of vascular access for medium-term treatments compatible with peripheral perfusion.
Midline catheters must be placed by trained and specialised personnel. Although handling and maintenance do not require the intervention of a vascular access specialist, a series of requirements must be met to ensure proper functioning.
Definition of the midline catheter
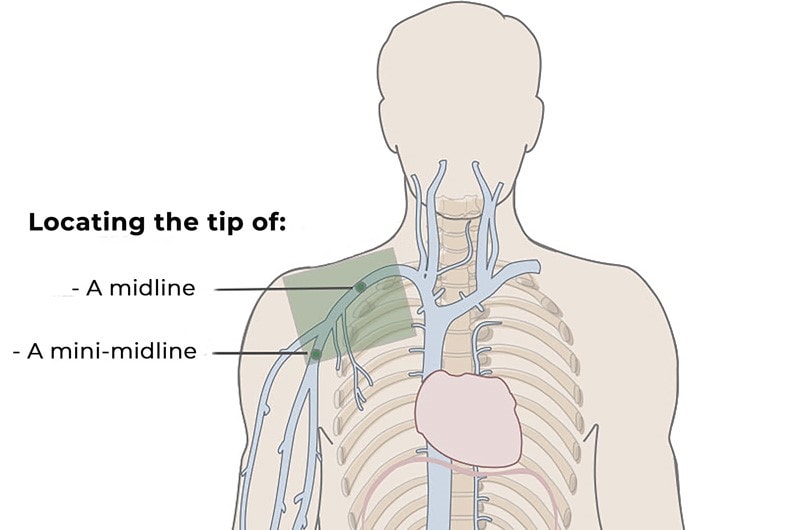
According to the GAVeCeLT manual on PICCs (peripherally inserted central catheters) and midline catheters, there are two types of midlines:
• Mini-midline: 8-10 cm catheter that can be inserted in the forearm or arm with a tip position that does not go beyond the axillary cavity.
• Midclavicular (or clavicular) midline (or echo-midline): 20-25 cm catheter that is always inserted in deep veins of the arm with the tip positioned in the thoracic section of the axillary vein or up to the subclavian vein.
Indications
A midline must be placed in the following cases:
• Poor peripheral venous tree; DIVA patients
• Temporary access while awaiting final access
• Administration of electrolytes, feeding aid with osmolarity < 800-850 mOsm/L (1)
• Core therapy involving complications
• Osmolarity < 800-850 mOsm/L (1) and/or pH between 5-9
• Treatment > 7 days
• Antibiotic therapy in serious infections: endocarditis, osteomyelitis
• Blood collection (2)
• Blood transfusion
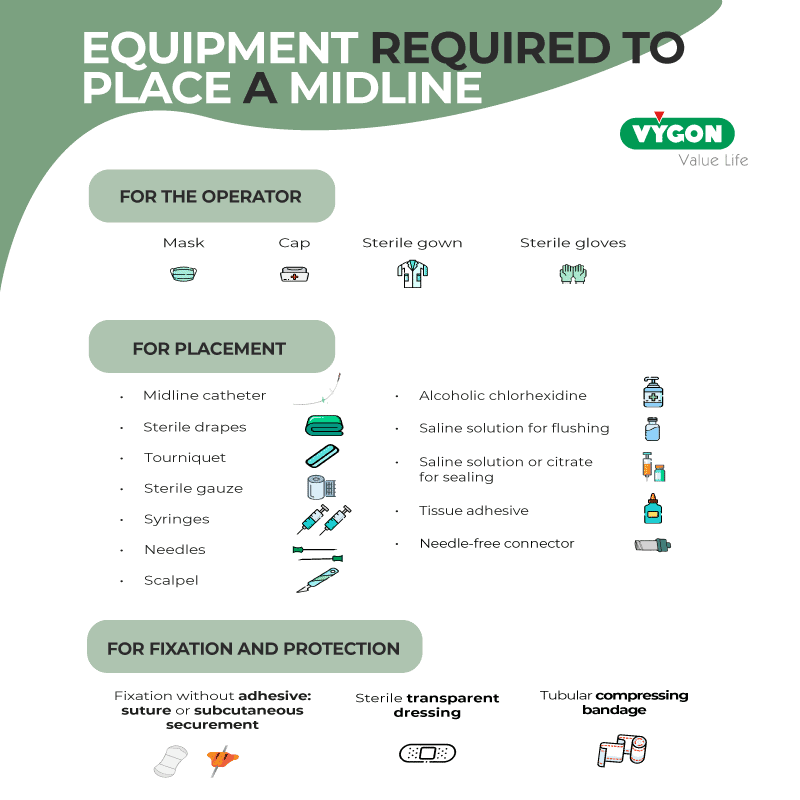
Necessary material
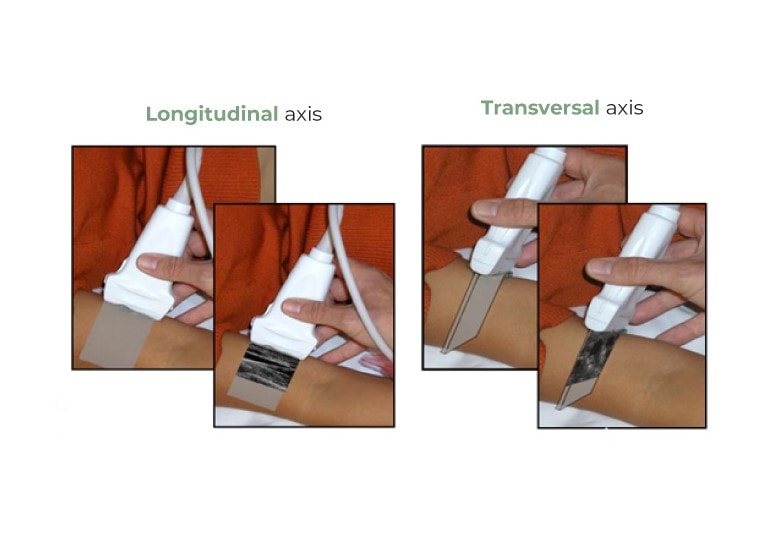
Ultrasound examination
The insertion site is the upper limb—specifically in the middle third of the arm (basilic, brachial and cephalic veins).
Previous ultrasound mapping is used to view the veins in this area (even at shoulder level) in the transverse or longitudinal axis, depending on the position of the probe. For this purpose, it is recommended to use the RaPeVA method (from the GAVeCeLT group) to perform a rapid ultrasound assessment of the peripheral veins.
What to avoid
• Flexures
• Veins with the presence of phlebitis
• Thrombosed or varicose veins
• Limbs with lymph node dissection
• During the recognition of structures, rule out the Mickey Mouse area: the course of the brachial artery (Mickey Mouse’s head) runs very close to the brachial veins (Mickey Mouse’s ears) that may be options for cannulation. However, in this section, it is not recommended since the artery and the median nerve are very close.
Midline Installation technique
This ultrasound-guided technique makes it possible to cannulate deep veins of the arm such as the basilic, brachial and cephalic, depending on the course and calibre.
Insertion
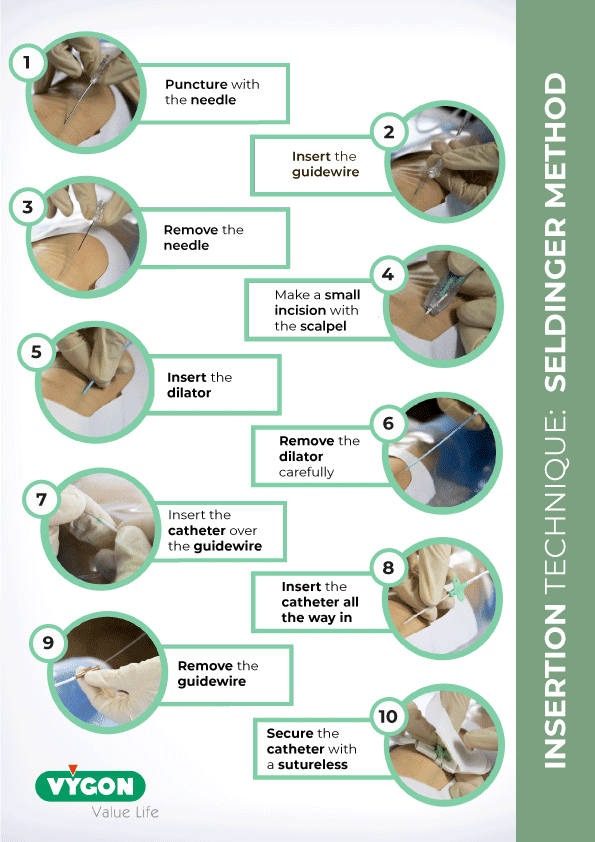
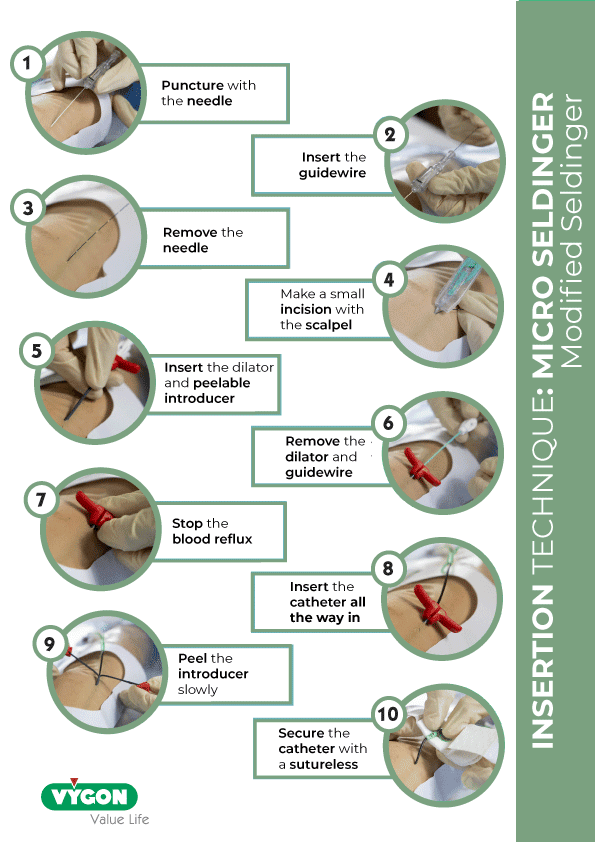
There are two insertion techniques: the Seldinger and the Micro Seldinger technique.
Process
> Before preparation:
• Active identification of the patient
• Inform the patient of the procedure to be followed
> Preparation:
1. Handwashing
2. Place the patient in a supine position with the arm at a right angle to the chest.
3. Ultrasound mapping (RaPeVA) and vein selection
4. Handwashing
5. Asepsis of the skin, washing with chlorhexidine soap and non-sterile gloves, change of gloves, disinfection with alcoholic chlorhexidine (handwashing between the two sequences)
6. Placement of cap and surgical mask and handwashing
7. Preparation of the sterile field
8. Handwashing
9. Gloves and sterile gown
10. Apply the tourniquet
Placement
1. Puncture of the selected vein according to the ultrasound-guided technique, then, insertion of the catheter
2. Cleaning of the venipuncture site
3. Connection of the bioconnector, flushing with 10 ml of saline solution using the push-pause-push technique and positive pressure
4. Locking with saline solution or citrate depending on the protocol of the service with a volume equivalent to 120% of the dead space (internal volume) of the catheter
5. Catheter fixation with an adhesive or subcutaneous anchoring system
6. Locking of the insertion point with tissue adhesive
7. Transparent sterile dressing
8. Record procedure
Midline catheter maintenance
Maintenance dressings are carried out every 7-10 days or when they get dirty, become loose, or contain blood.
Here are the steps to follow:
1. Change dressing and needle-free connector
2. Check position, reflux, catheter status and insertion point
3. Flush with 10 ml of saline solution (push-pause technique with positive pressure)
4. Lock with saline solution or citrate according to the protocol of the institution (with the same technique as above)
5. Record the procedure in the computerised clinical history.
The most common midline complications are phlebitis, infection, occlusion, thrombosis, extravasation, and skin lesions.
Midline catheter removal
Catheter removal is a simple procedure and must be carried out in the following cases:
• Catheter not necessary or unsuitable
• Infection
• Irreversible obstruction
• Mechanical injury
• Venous thrombosis with malfunction
• Malfunction due to fibrin sheath or other reasons
The procedure consists of following strict asepsis measures, culturing the tip of the catheter (in case of infection) and recording the data in the patient’s file.
BIBLIOGRAPHY
- Pittiruti and Scoppettuolo, GAVeCeLT Manual on PICC and midline, Edra edition – 2016
- GAVeCELT Group, DAV Expert website, 2016 – accessed March 2021
- Infusion Nursing Society, Infusion Therapy Standards of Practice – 2021
- CDC Recommendations – 2011
- Ministry of health, social services and equality, Clinical Practice Guideline on Intravenous Therapy with Non-Permanent Devices in Adults – 2014




