
PICC-port is an implanted catheter that is undoubtedly gaining ground in the world of vascular access. Its growing success is not surprising: it comes with new indications, cost reduction and patient satisfaction.
Even if PICC-port has been in use for several decades, it is only in recent years that it has gained momentum among new technologies and best practices in the field of vascular access.
Ports placed in the forearm or arm using invasive techniques such as the Seldinger technique or fluoroscopy are outdated concepts that have been surpassed by recent advancements in both techniques and materials. This is where the PICC-port excels; by leveraging these safe techniques and minimizing vascular damage and complications, it can ultimately reduce costs.
Furthermore, PICC-port functions as a hybrid catheter as it is placed like a PICC but exhibits the characteristics of a port. It also encompasses a comprehensive nursing procedure that goes from assessment to removal.
PICC-PORT INDICATIONS
The indications for the placement of PICC-ports are very broad, and as new scientific evidence emerges, they continue to expand. It would not be surprising if, in a few months, thanks to scientific literature, the indications translate into new possibilities.
- TYPE OF TREATMENT
PICC-ports are used with patients who require long-term treatment (over 3 months) with an estimated frequency of less than once a week. A clear example of this type of treatment is chemotherapy.
Initially, the insertion of a PICC-port was not recommended when home infusion through an elastomeric pump was scheduled. However, once again, professional experiences and evidence tell us that the use of elastomeric pumps through a PICC-port at home is safe and feasible for patients who have suitable medical support.
- CHARACTERISTICS OF THE PUNCTURED VEIN
Given that the insertion of a PICC-port is identical to that of a PICC-line (involving the use of ultrasound guidance and modified Seldinger technique in the deep veins of the arm), the assessment criteria for PICC-port insertion remain the same as those for a PICC. This entails ensuring the use of veins with the adequate size in relation to the catheter’s French size, as well as a safe positioning of the vein to avoid any potential damage to surrounding structures, such as nerves and arteries.
- SPECIFICITY OF THE PATIENT
PICC-ports are suitable for patients with a tracheostomy, or a chest or neck wound due to radiotherapy, surgery, complex injury, or other clinical conditions that affect the integrity of the skin in the head, neck, or chest area.
For patients undergoing radiation therapy as a future treatment, the catheter can remain in place throughout the treatment period. Similarly, patients undergoing treatments that lead to wounds in the head, neck, or chest such as cetuximab treatment that causes folliculitis in those areas, can benefit from the insertion of a PICC-port.
- PATIENT’S PREFERENCE
Some patients, particularly young women who have undergone abdominal or thoracic surgeries resulting in visible scars, may prefer not to have a catheter in their chest to avoid additional scars on their trunk.
In such cases, the expert DAV (Direct Antiviral Agents) algorithm provides a conceptual map to guide healthcare professionals in choosing the most suitable vascular access option. It recommends a step-by-step approach for selecting a PICC-port, with the first preference being a catheter placed in the arm due to its low complication rate.
PICC-PORT CONTRAINDICATIONS
The contraindications of a PICC-port are also aligned with the contraindications of a PICC.
- AXILLARY LYMPH NODE DISSECTION
If it is unilateral, the opposite side can be considered, but if it is bilateral, the PICC-port is absolutely contraindicated.
- INADEQUATE VEINS
There is no suitable vein in the arm in terms of size, position, collapsibility, and depth.
- SUPERIOR VENA CAVA SYNDROME
Obstruction or compression of the superior vena cava, mainly due to a tumour, prevents the use of a PICC-port.
- RENAL INSUFFICIENCY
When it comes to chronic renal insufficiency in stage 3b-4 that will require the creation of an arteriovenous fistula in the future or if there is already a fistula in the arm.
- TYPE OF TREATMENT
When a long-term continuous home infusion treatment is anticipated, such as parenteral nutrition.
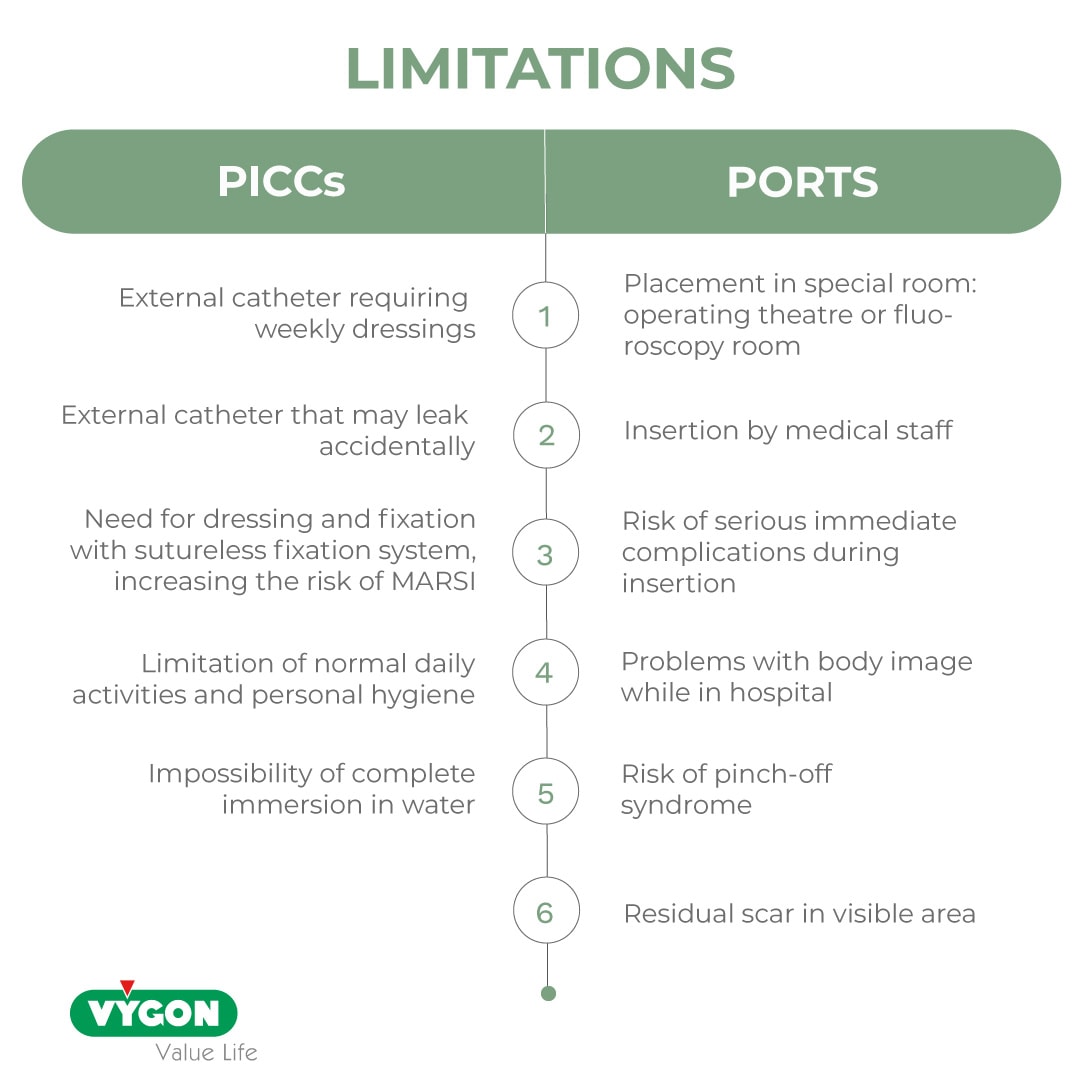
PICC-PORT ADVANTAGES OVER PICC AND CHEST PORT
The placement of a PICC-port in the arm offers several advantages compared to a chest port, not only for patients but also for institutions.

Compared to the disadvantages that other central catheters may have, PICC-ports offer several advantages:
- They are fully implanted catheters under the skin that do not require weekly dressings and have no risk of accidental dislodgment.
- They are placed in clean rooms using catheter tip verification techniques that do not involve radiation.
- They are inserted by a specifically trained nursing staff. The entire procedure from assessment to catheter removal can be considered as part of nursing process.
- They do not have serious immediate complications during insertion. The use of ultrasound by experienced professionals ensures successful puncture and eliminates the risk of relevant complications. Late complications, such as thrombosis, are similar to those associated with a chest port placed using ultrasound, except for pinch-off syndrome, which is completely eliminated, as well as hematoma.
- They enhance patient satisfaction for several reasons: reduced emotional stress due to the placement site (arm rather than chest), reduced potential for complications, small size and minimal scarring in less visible areas improve aesthetics and body image, enable a normal lifestyle as a fully implanted catheter does not limit normal activities and allows a regular personal hygiene.
It is crucial to emphasize that the insertion of this catheter should be performed by prepared and properly trained nurses. The insertion technique for this catheter corresponds to that of a PICC, with the difference being the creation of a subcutaneous pocket and tunnelling. Both procedures are easy to learn and execute for nursing personnel, whose professional curriculum, skills, and abilities may include performing complex dressings, minor surgeries, and suturing once they have received appropriate training.
As always, evaluating the effectiveness of a device solely based on its market price is not correct. Therefore, we need to calculate the cost-effectiveness of PICC-ports based on the following parameters:
- Nursing procedure: ultrasound assessment, patient interview, insertion, follow-up, resolution of potential complications, and removal.
- Insertion context: in non-specific rooms, without the need for radiation.
- Elimination of serious immediate complications and reduction of late complications: entirely manageable by trained nurses.
- Patient satisfaction resulting in fewer unnecessary visits to the emergency department.
Failure to recognize the PICC-port procedure as a new nursing competency would result in the loss of a crucial aspect of this technique and the associated advantages.
“Institutions that begin to implement PICC-ports should consider the procedure as part of the activities of Vascular Access Nursing Units (ETI, UTI, etc.) as a short and long-term cost-saving strategy that is meant to increase patient satisfaction.”
BIBLIOGRAPHY
- Infusion Therapy Standards of Practice. Journal of Infusion Nursing. 2021.
- Merlicco D, Lombardi M, Fino MC. PICC-port: valid indication for placement in patients with extensive burns of the neck and chest in oncology. The first case in the scientific literature. IJSCR. 2020. 63-66.
- Biffi R, Pozzi S, Bonomo G, Della Vigna P, Monfardini L, Radice D, Rotmensz N, Zampino MG, Fazio N, Orsi F. Cost effectiveness of different central venous approaches for port placement and use in adult oncology patients: evidence from a randomized three-arm trial. Ann Surg Oncol. 2014; 21(12):3725-3731.
- Kreis H, Loehberg CR, Lux MP, Ackermann S, Lang W, Beckmann MW, Fasching PA. Patients’ attitudes toward totally implantable venous access port systems for gynecological or breast malignancies. Eur J Surg Oncol. 2007; 33:39-43.
- Bertoglio S, Cafiero F, Meszaros P, Varaldo E, Blondeaux E, Molinelli C, Minuto. PICC-port totally implantable vascular Access device in breast cancer patients undergoing chemotherapy. (2019) J Vasc Access. Nov 1:1129729819884482 (ahead of print)
- Yang S, Ahn M. A comparison between the upper arm and chest for the optimal site of totally implanted venous access ports in patients with female breast cancer. Ann Vasc Surg. 2018; 50:128-134.




