Central venous catheters (CVCs) are essential tools in modern medicine, providing reliable vascular access for fluid administration, medication delivery, and haemodynamic monitoring. However, CVC insertion can be a resource intensive procedure with potential for serious complications such as perforation, tamponade, and malposition. Traditionally, chest X-ray (CXR) has been the gold standard for confirming proper CVC tip placement in the lower third of the superior vena cava (SVC), aiming to minimise these risks.
While CXR remains valuable, it introduces delays, radiation exposure, and increased costs. Emerging evidence supports electrocardiogram (ECG)-guided CVC tip placement as a viable and advantageous alternative. This article explores the benefits and methodology of ECG-guided CVC placement, highlighting its potential to improve patient safety and streamline clinical workflows.
Leveraging ECG-Guided CVC Placement:
ECG-guided CVC placement leverages the electrical activity of the heart to determine the catheter tip’s location in real-time. By monitoring the P-wave morphology, clinicians can accurately position the catheter within the SVC, reducing the need for routine CXR confirmation in uncomplicated insertions.
Key Advantages:
- Real-time feedback: ECG provides immediate feedback, allowing for precise catheter manipulation and optimal positioning.
- Reduced radiation exposure: Minimises or eliminates the need for post-procedural CXR, reducing radiation exposure for both patients and staff.
- Time efficiency: Streamlines the procedure, reducing delays and allowing for faster initiation of therapy.
- Cost-effectiveness: Reduces the need for costly radiological imaging.
- Accuracy and safety: Studies have demonstrated that ECG-guided placement is comparable to, and in some cases more accurate than, anatomical landmark techniques, and is a safe procedure.
The ECG-Guided Technique: A Step-by-Step Guide
Equipment Required:
- Universal ECG adapter
- Lead cable from the ECG monitor
- Disposable cable
- Guidewire
- Red skin electrode
Procedure:
1. Preparation
- Gather Equipment: Ensure you have all necessary equipment, including the CVC kit, ECG monitor, sterile gloves, drapes, and antiseptic solution.
- Patient Positioning: Position the patient in a supine position with the head slightly tilted to the opposite side of the insertion site.
- Sterilisation: Perform hand hygiene and establish a sterile field. Clean the insertion site with an antiseptic solution and allow it to dry.
2. Insertion Site Selection
- Identify the Vein: The internal jugular vein is commonly used for CVC insertion. Use ultrasound guidance if available to locate the vein and mark the insertion site.
3. Needle Insertion
- Insert the Needle: Insert the needle into the vein at the marked site. Confirm venous access by aspirating blood.
4. Guidewire Insertion
- Advance the Guidewire: Insert the guidewire through the needle and advance it into the vein. Ensure the guidewire moves smoothly without resistance.
5. Catheter Insertion
- Dilate the Tract: Remove the needle and use a dilator to enlarge the tract. Then, advance the catheter over the guidewire into the vein.
- Remove the Guidewire: Once the catheter is in place, partly remove the guidewire while maintaining control of the catheter.
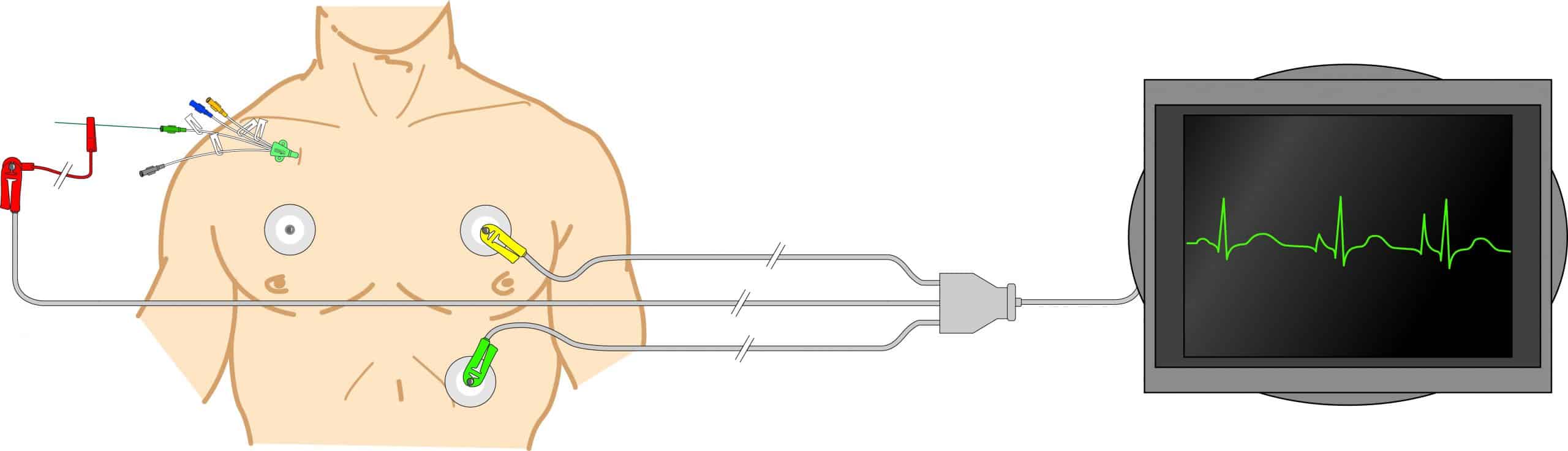
6. ECG Monitoring
- Connect the ECG: Attach the ECG cable to the guidewire. The crocodile clip should be connected to the guidewire’s “J” tip, which protrudes from the distal end of the catheter.
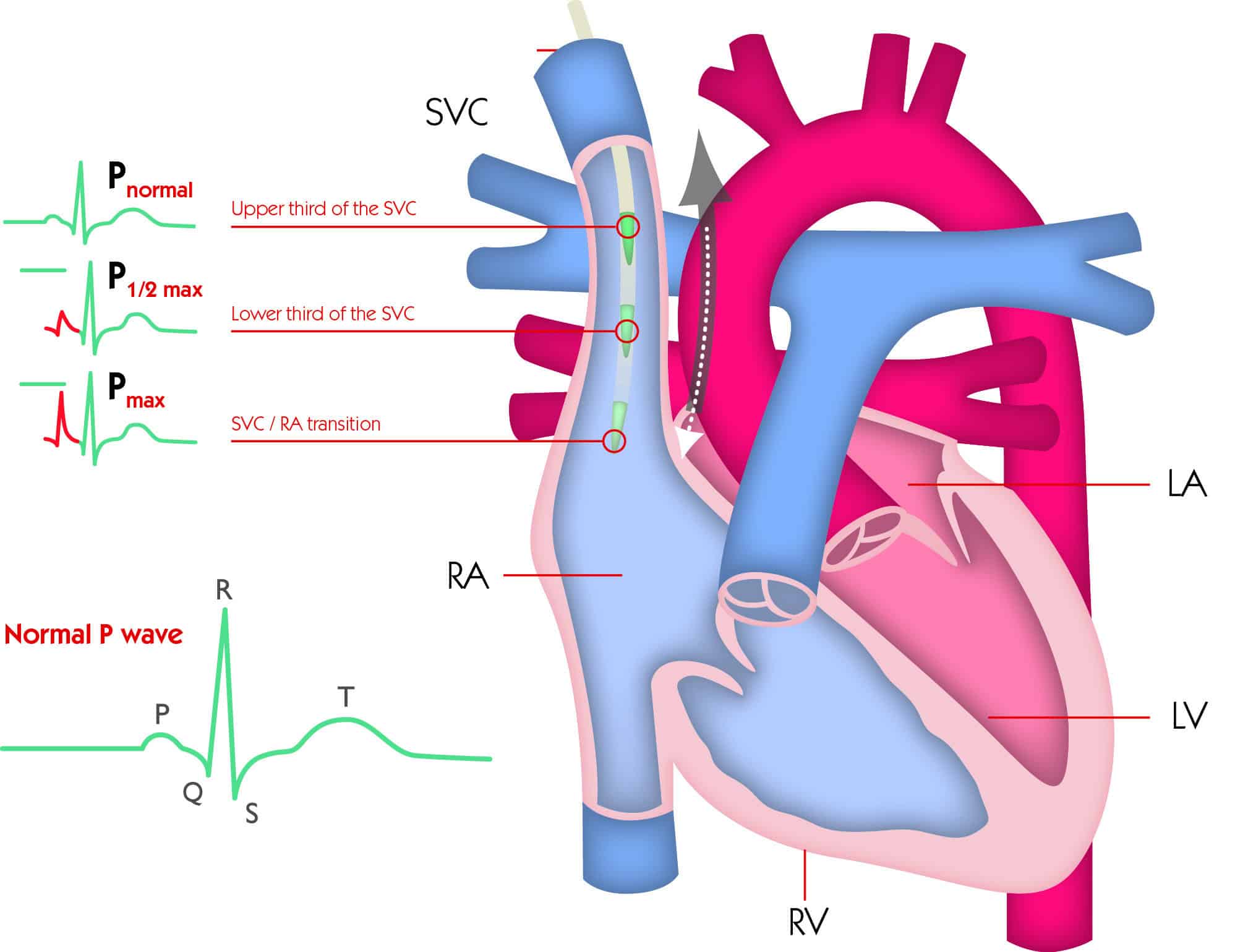
- Monitor the P-Wave: As the catheter tip advances towards the superior vena cava (SVC) and right atrium, observe the P-wave morphology on the ECG monitor. The P-wave amplitude will increase as the catheter approaches the right atrium.
- Optimal Positioning: The correct position is indicated when the P-wave is at its highest amplitude without becoming biphasic. If the P-wave shows negative features, withdraw the catheter slightly.
7. Confirmation and Securing
- Confirm Placement: Once the catheter is in the correct position, confirm the placement using the ECG monitor.
- Secure the Catheter: Secure the catheter with sutures or a manufactured securement device. Apply a sterile dressing over the insertion site.
8. Post-Procedure Care
- Flush the Catheter: Flush the catheter lumens with saline to ensure patency.
- Monitor the Patient: Observe the patient for any immediate complications and ensure the catheter is functioning correctly.
Clinical Implications and Considerations:
ECG-guided CVC placement offers a valuable alternative to traditional CXR confirmation, particularly in uncomplicated insertions. However, it’s crucial to acknowledge that:
- Clinicians must be adequately trained and proficient in ECG interpretation and the technique.
- CXR confirmation may still be necessary in certain situations, such as difficult insertions, suspected complications, or in patients with pre-existing cardiac abnormalities that affect ECG interpretation.
- This technique is not a replacement for good clinical judgement.
Conclusion:
ECG-guided CVC tip placement represents a significant advancement in vascular access procedures. By offering real-time feedback, reducing radiation exposure, and improving efficiency, this technique has the potential to enhance patient safety and optimise clinical outcomes. As evidence continues to support its efficacy, ECG-guided CVC placement should be considered a valuable tool in modern clinical practice.
References
- Krishnan AK, Menon P, Gireesh Kumar KP, Sreekrishnan TP, Garg M, Kumar SV. Electrocardiogram-guided Technique: An Alternative Method for Confirming Central Venous Catheter Tip Placement. J Emerg Trauma Shock. 2018 Oct-Dec
- Booth S A, Norton B, Mulvey D A. Central venous catheterization and fatal cardiac tamponade. BJA: British Journal of Anaesthesia, Volume 87, Issue 2, 1 August 2001,
- de Man L, Wentzel M, van Rooyen C, Turton E. Comparison between ultrasound and chest X-ray to confirm central venous catheter tip position. SA J Radiol. June 2023


