Optimising Outcomes Through Proper Device Selection
Arterial cannulation is not just about technique—it’s also about choosing the correct device for the right patient. The type, size, and design of the arterial catheter can significantly influence the accuracy of monitoring, the risk of complications, and the overall success of the procedure. In this section, we explore how to make informed decisions about device selection to ensure optimal outcomes.
Why Device Selection Matters
Arterial lines are used primarily for:
- Continuous blood pressure monitoring
- Frequent arterial blood sampling
But not all devices are created equal. Factors such as dwell time, signal quality, and patient-specific risks must be considered when selecting a catheter.
Indications and Contraindications
Indications for arterial line placement include:
- Continuous and accurate blood pressure monitoring
- Frequent arterial blood sampling for blood gas analysis.
- Avoiding repeated needle sticks in critically ill patients
Contraindications There are no absolute contraindications to arterial line placement, but if any of the below are present, then senior medical opinion should be sought before proceeding
- Thromboangiitis obliterans (Buerger disease)
- Raynaud’s syndrome
- Atherosclerosis
- Coagulopathy
- Inadequate collateral flow
- Infection at the cannulation site
- Burn at the cannulation site
- Previous surgery in the area
- Synthetic vascular graft
- Presence of AV fistula.
Understanding Dwell Time
The expected duration of arterial line use should guide your device choice:
- Short-term use (hours to 1–2 days): A standard cannula may suffice.
- Longer-term use (several days): A Seldinger catheter is preferred due to its longer length and reduced risk of dislodgement.
💡 Seldinger catheters have been shown to maintain accurate pressure readings and reliable access for longer periods compared to shorter cannulas.
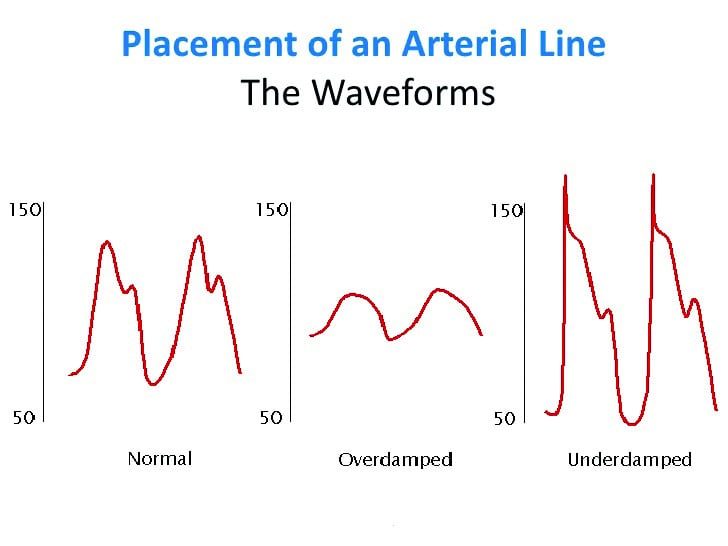
Signal Quality: The Damping Dilemma
When using an arterial line for continuous blood pressure (BP) monitoring, signal quality is crucial. Poor signal transmission can lead to inaccurate readings and clinical misjudgements.
- Over-damping: Causes underestimation of systolic and overestimation of diastolic pressure.
- Causes: Bubbles, clots, kinks, long/narrow tubing.
- Under-damping: Causes overestimation of systolic and underestimation of diastolic pressure.
- Causes: Rigid, non-compliant tubing.
Solution: Use a catheter with the correct gauge and pliancy. A 20G catheter is typically ideal for the radial artery in adults—wide enough to reduce the risk of thrombus, yet small enough to preserve vessel integrity.
The Top Device Options
There are several options available; however, fundamental arterial line systems should include the following:
Option one
- Classic Seldinger technique
- Polyethylene material for accurate waveform
- Red hub for easy identification
Option two
- Non-Seldinger (over-the-needle) arterial cannula
- Direct insertion with integrated flashback for rapid confirmation
- Simplified design for quick deployment in routine cases
These systems are designed to support both clinical accuracy and safety.
Clinical Tips for Device Selection
- Match catheter length and gauge to the artery and patient size.
- Choose a device that supports critical damping for accurate waveform.
- Consider blood sampling needs—some systems are better suited for frequent draws.
- Always prime the system and check for air bubbles before connection.
Conclusion
Device selection is a critical, often underappreciated, component of arterial line placement. By aligning your choice with the patient’s clinical needs, expected dwell time, and anatomical considerations, you can improve accuracy, reduce complications, and enhance patient safety.