Central venous catheters are one of the most commonly used devices in hospitals, however, they can present some complications, and to avoid them, proper care and maintenance of the device is essential.
WHAT WILL YOU FIND IN THIS ARTICLE?
- Monitoring of the insertion site
- Healing of the insertion site
- Dressing placement
- Maintenance of infusion systems and accessories
- Catheter flushing and catheter patency
- Catheter change
- Bacteremia Zero
Want to know more about CVC maintenance and care? Stay on this page and read the full post.
Central venous cannulation is a common procedure, however, it does present some risks. The complications that can be encountered are mechanical, infectious and thrombotic.
Mechanical complications are largely operator-dependent and most are detected at the time of catheter insertion. Infectious and thrombotic complications usually occur after insertion and this is where care and maintenance of the device plays a key role.
To avoid late central venous catheter-related complications, we will address recommendations and best practices to reduce potential health risks to the patient, which we will divide into 6 key moments:
- Monitoring of the insertion site
- Healing of the insertion site
- Dressing placement
- Maintenance of infusion systems and accessories
- Catheter flushing and catheter patency
- Changing the catheter
1. MONITORING OF THE INSERTION ZONE
After insertion of the central venous catheter, nursing should monitor the site in order to avoid complications associated with the device. To identify possible risks, the following should be done:
- Monitor the insertion site of vascular catheters daily without removing the dressing for signs of alarm (erythema, pain, oozing, etc.). 9
- Do not use antibiotics or topical antiseptic ointment to protect the insertion site. 9
- Sterile semi-permeable transparent dressings should be used, so that the insertion site can be assessed with as little manipulation as possible. 9
- The date of dressing placement and dressing cure should be recorded both in the nursing records and near the dressing. 9
2. HEALING OF THE INSERTION SITE
Most catheter-associated infections are related to skin colonisation. Therefore, daily care of the CVC insertion site is of great importance. The area should be kept dry, clean and free of contamination. 2
The skin should be disinfected with an appropriate antiseptic prior to catheter insertion and during dressing changes. 4
The most recommended solution is a 2% aqueous or 0.5% alcoholic chlorhexidine preparation. 4
3. DRESSING PLACEMENT
Dressings are an essential element to help keep CVCs and their insertion site clean and dry. The most commonly used dressings are composed of an adherent transparent polyurethane film. They have the advantage of allowing constant inspection of the site to identify local infection, pressure damage or other visible complications at the insertion site without the need to change the dressing. 2
Central line dressings should not be changed every day unless they are loose or soiled. Current recommendations are to change the gauze dressing every two days and the transparent semi-permeable dressing every seven days, unless it is soiled or loose. 2
If the patient is diaphoretic, bleeding or oozing at the insertion site, a gauze dressing should be used until the problem is resolved. 2
AVOIDING MARSI
To avoid problems such as MARSI, i.e. skin lesions related to the dressing or skin adhesive, a correct dressing application and removal technique must be used:
- Assess the skin before applying any adhesive and record risk factors to be taken into account.
- Follow the natural Langer’s lines of the skin.
- Allow disinfectant to dry completely.
- Never remove hair by shaving.
- Do not touch the adhesive side with your hands before applying the dressing.
- Leave the dressing on the skin, never tighten it.
- Use skin protectant (recommended).
- Apply light pressure and heat after dressing has been applied.
- Check dressing for patency and flexibility for patient comfort.
- Remove dressings at a slight angle and in a gentle manner in favour of the hair.
- Always make a record of the assessment and status of the dressing.

4. MAINTENANCE OF INFUSION SYSTEMS AND ACCESSORIES
To avoid infection and possible complications associated with the central venous catheter, it is also important to pay attention to the infusion system and its accessories by changing the infusion system and additional devices:
- For the handling of equipment, key connections and bioconnectors, hygienic hand washing and the use of clean gloves must be carried out. 8
- As few three-way taps as possible shall be used and free lights shall always be protected by their corresponding plug. 8
- A single light of the three-way valves shall be used to place a bioconnector, through which bolus and discontinuous solutions shall be administered. This door shall be previously protected by a plug impregnated with alcohol solution or the area shall be disinfected with alcohol solution for 30 seconds. 8
- and whenever the connections are visibly dirty or in case of accidental disconnections. 8
- Identify on IV systems when the IV is changed.
- Whenever a catheter is changed, all infusion sets, extension sets and other accessories shall also be changed. 8
- Perfusion of lipid-containing fluids must be terminated within 24 hours of initiating the infusion. 8
- Choose and designate a dedicated light for Parenteral Nutrition. 8
- Change parenteral nutrition equipment and other lipid emulsions every 12 – 24 hours. 8
5. CATHETER FLUSHING AND PATENCY
Maintenance of catheter patency is essential for all types of venous catheters and is probably the most crucial factor in preventing device malfunction and preventing occlusion.
Causes of catheter occlusion can be thrombotic, related to drugs or parenteral nutrition (PN) precipitates, or mechanical. Thrombotic obstruction is caused by an intraluminal clot or thrombus at the catheter tip. Precipitates may be formed by drug mixtures at extreme pH, calcium phosphate crystals or lipid deposits. 5
Flushing and sealing of the device lumen should be performed according to the protocol of the centre where the device is located. However, generally speaking, the recommended flushing technique for central venous catheters is in pulses (1ml at a time), the maintenance of positive pressure creates turbulence within the catheter lumen which aids in the removal of particles on the catheter wall. 6
When flushing the CVC, 10ml syringes should be used to avoid creating increased pressure that may contribute to catheter rupture due to excessive pressure. 6
Regarding the solution used, in adult central venous catheters, the difference between the use of heparin or saline is minimal, heparin has shown less occlusions, but the quality of evidence is low. There are no differences in terms of duration of patency and safety outcomes such as sepsis, mortality or bleeding. 7
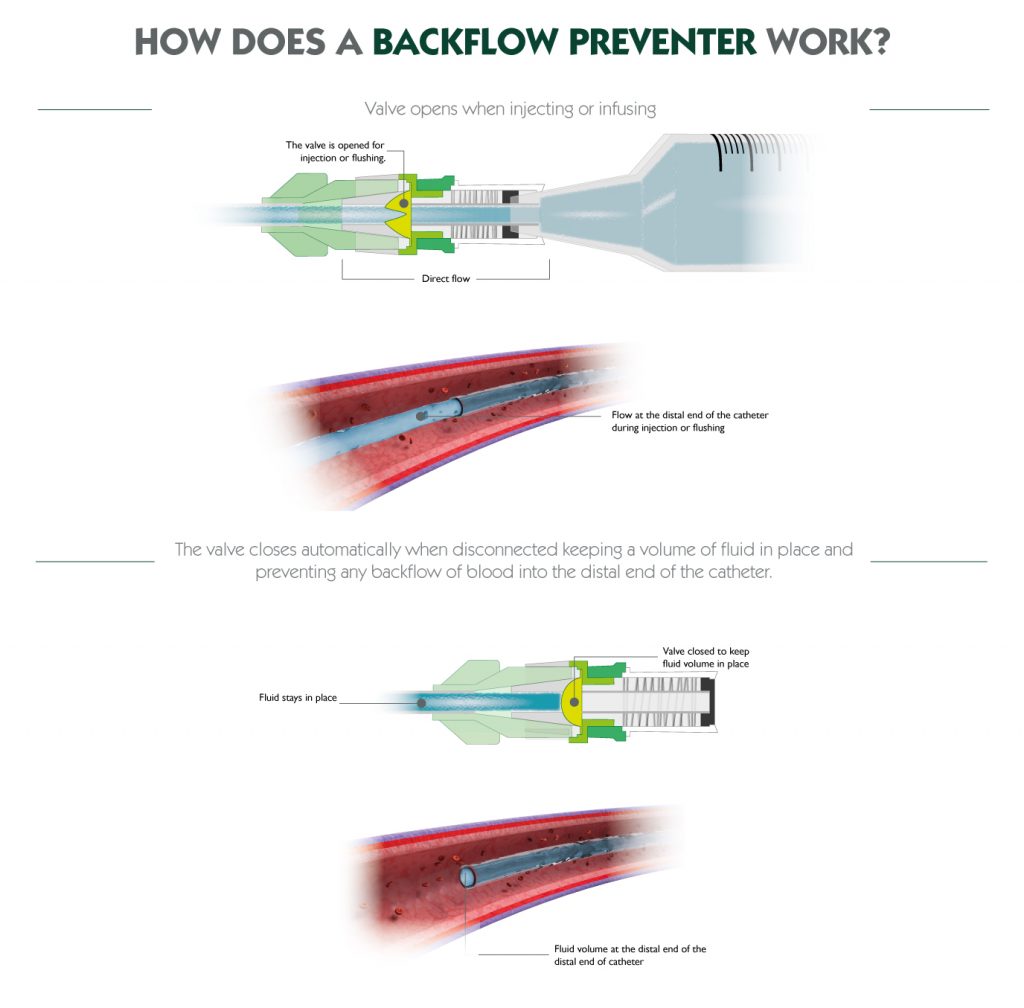
Finally, it is also useful to incorporate anti-reflux valves. This is a bi-directional fluid control valve, which remains closed until the infusion or withdrawal force reaches a specified pressure and, as the infusion or withdrawal pressure begins to reduce, the valve closes again.
Currently, the anti-reflux connector is the only device that prevents blood from entering the catheter in all these circumstances.
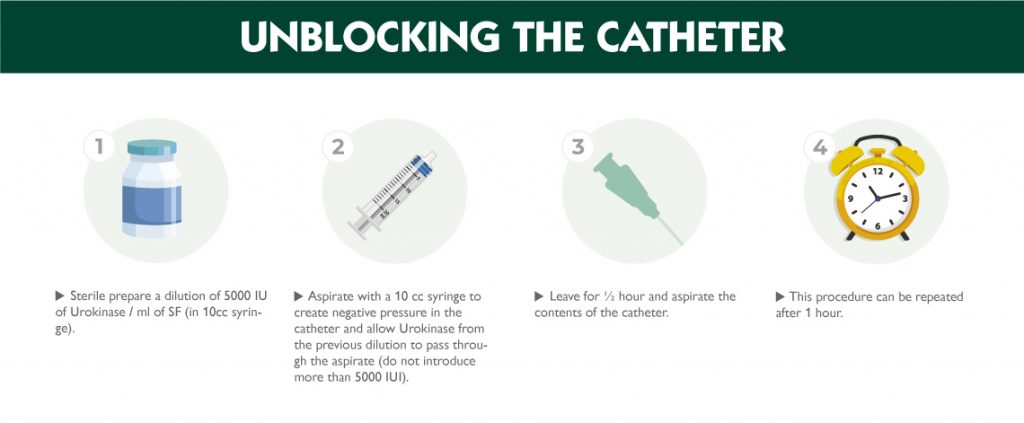
UNBLOCKING THE CATHETER
If the catheter is blocked, Urokinase can be used to restore patency.9
- Sterile prepare a dilution of 5000 IU of Urokinase / ml of SF (in 10cc syringe). 9
- Aspirate with a 10cc syringe to create negative pressure in the catheter and allow Urokinase from the previous dilution to pass through aspiration (do not introduce more than 5000IU). 9
- Leave for ½ hour and aspirate the contents of the catheter. 9
- This procedure can be repeated after 1 hour. 9
- Before performing this procedure, consult your doctor.9
6. CATHETER CHANGE
Central catheters should not be replaced routinely. Again, however, it is important to monitor for local and systemic signs of infection.
- Catheter duration is related to correct insertion technique. 3
- Remove any catheter that is not absolutely necessary. 8
- When catheter insertion is urgent and sterile technique cannot be used, it is recommended that the catheter be changed within 48 hours and a new catheter placed in a different location. 8
- CVCs should be changed if oozing is observed at the insertion site.3
- Do not perform catheter exchange through guidewire in CVCs suspected of having a catheter-related infection. 3

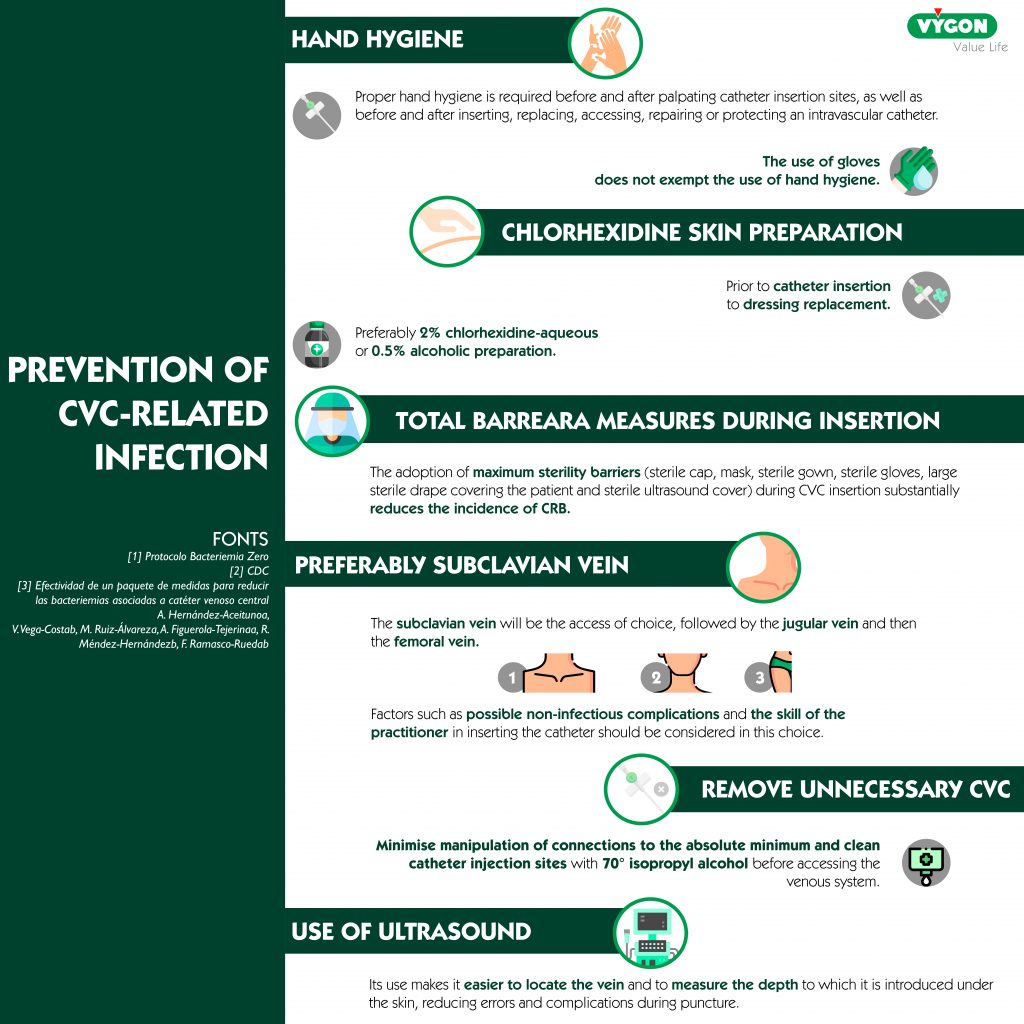
BACTERAEMIA ZERO PROTOCOL
In addition to the above points, the Bacteraemia Zero Protocol must also be implemented. The main objective of this project at its inception was to reduce the state average catheter-related bacteraemia (CRB) rate to less than 4 episodes of bacteraemia per 1,000 CVC days.
Thanks to this initiative, CRB has been reduced, but even after more than ten years it continues to be a major problem.
This project brings together recommendations on:
- Insertion
- Maintenance
- Patient hygiene
- Catheter removal and changes
- Use of ultrasound for catheter insertion
BIBLIOGRAPHY
- Hull, G. J., Moureau, N. L., & Sengupta, S. (2018). Quantitative assessment of reflux in commercially available needle-free IV connectors. The Journal of Vascular Access. Published. https://doi.org/10.5301/jva.5000781
- Ball M, Singh A. Care Of A Central Line. . In: StatPearls . Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK564398/
- Cayón, J. D., Iza Castanedo, V., Monje Álvarez, A., San Emeterio Pérez, C., Soler Dorda, G., Camus Burgueño, E., Fuentevilla Montes, R., Barquín Pomar, G., Martínez Ochoa, E., Moreno De La Hidalga, M. a. Á., Antolín Juárez, F., Gomez Cosío, L., Gomez Peral, P., Hernández Hernández, M. Á., Maestre Alonso, J. M., & Díaz Mendi, A. R. Guía para la inserción y mantenimiento de catéteres. https://www.scsalud.es/c/document_library/get_file?uuid=690873bd-bc46-4bc4-96db-a01818abc7ed&groupId=2162705
- Bacteriemia Zero. Protocolo prevención de las bacteriemias relacionadas con catéteres venosos centrales (brc) en las uci españolas (2015). Plan de Calidad para el Sistema Nacional de Salud. Ministerio de sanidad y consumo de España. https://seguridaddelpaciente.es/resources/documentos/2015/PROTOCOLO_BACTERIEMIA_ZERO.pdf
- Goossens, G. A. (2015). Flushing and Locking of Venous Catheters: Available Evidence and Evidence Deficit. Nursing Research and Practice, 2015, 1–12. https://doi.org/10.1155/2015/985686
- Manual de protocolos y procedimientos generales de enfermería. Catéter venoso central: inserción, mantenimiento y retirada. (2010). Hospital Universitario Reina Sofía.https://www.sspa.juntadeandalucia.es/servicioandaluzdesalud/hrs3/fileadmin/user_upload/area_enfermeria/enfermeria/procedimientos/procedimientos_2012/h1_cateter_venoso_central.pdf
- Gómez Urquiza, J. L. (2021). ¿Es mejor el uso de suero salino o la heparinización en catéteres de vía venosa? Salusplay. https://www.ocez.net/archivos/noticia/1468-0.pdf
- Cuidados de Enfermería en los Accesos Vasculares Guía de Recomendaciones. Complejo Hospitalario Universitario de Badajoz.SE.
- PROTOCOLO DE CANALIZACIÓN, MANTENIMIENTO Y USO DE LA VÍA VENOSA CENTRAL DE ACCESO PERIFÉRICO (P.I.C.C.). https://www.chospab.es/publicaciones/protocolosEnfermeria/documentos/174984222e19f049e8476892f86be249.pdf
A place to learn about health procedures and techniques from leading professionals.




