What is Post-Dural Puncture Headache (PDPH) and when is active prevention indicated?
Post-Dural Puncture Headache (PDPH) is a positional headache that occurs within 5 days of a dural puncture, is relieved by lying down, and lasts ≤2 weeks or resolves following an epidural blood patch (EBP). 4
It occurs due to cerebrospinal fluid (CSF) leakage and is highly preventable by optimising the type of needle and the operator’s technique. 3-7
- Incidence: Varies from 0.5% to 25% or more, depending heavily on needle design, gauge and patient factors. 4–6
- Clinical impact: Causes debilitating pain, prolonged hospitalisation and frequent need for an epidural blood patch (EBP). 4–7–8
- Serious complications: Although rare, it can lead to subdural haematoma, cranial nerve palsy or arachnoiditis. 4-7.
- High-risk patients: Pregnant women, children, elderly people and low Body Mass Index (BMI). 4-7
Post-Dural Puncture Headache (PDPH) as a significant clinical problem
The primary objective of healthcare professionals is to guide patients towards a safe and smooth surgical recovery by promoting optimal pain control and reducing anesthesia-associated.
However, Post-Dural Puncture Headache (PDPH) remains a common and stressful complication that hinders this objective.
The impact of this complication goes far beyond a simple headache; it immobilises patients, delays the mother-infant bond in obstetrics and exponentially increases medical costs. 8-9
Modifiable risk factors: Needle type, technique and experience
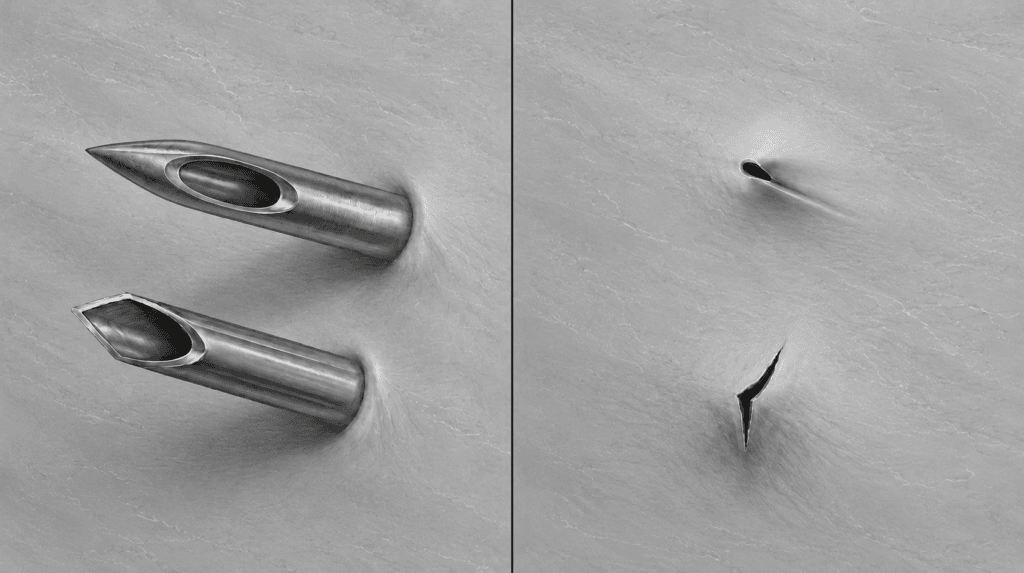
Needle bevel design
Cutting tip needle | Pencil point tip needle | ||
Design and Advantages | Risks and Disadvantages | Design and Advantages | Risks and Disadvantages |
It has a cutting bevel that facilitates a rapid flow of CSF during the puncture. 7 | Cuts the dural fibres, causing greater trauma and a higher incidence of PDPH (e.g. 8.5% with a 25G needle). 3-6 | It separates the fibres without cutting them, reducing trauma and facilitating closure of the dural opening. 3-6 | Very fine needles may make the technique difficult and require more attempts by the operator. 5-7 |
Context of Use Avoid in high-risk patients. If used, the bevel should be aligned parallel to the fibres. 4 | Context of Use Preferred choice, incidence <3% (with a 25G needle): ideal in obstetrics and for vulnerable patients. 3 | ||
Selecting an atraumatic pencil-tip needle is the most effective preventive measure to avoid Post-Dural Puncture Headache (PDPH), making this choice a direct decision regarding safety.3-6
Needle gauge
Using a smaller gauge (e.g. 25G or 27G) inherently reduces the overall risk of developing Post-Dural Puncture Headache (PDPH). 5–7
However, design matters more than gauge alone: a 27G cutting needle has a 5–12% Post-Dural Puncture Headache (PDPH) rate, compared with a 25G pencil point needle at <3%. 3–6
High-risk patients: Considerations and complications (Clinical nuances)
Some patients have an exceptional physiological vulnerability to cerebrospinal fluid (CSF) leakage.
Ignoring these factors can lead to severe morbidity and dissatisfaction, as well as long-term complications. 4–7
a. Pregnant women:They are at particularly high-risk because of their young age, female gender, and the frequent use of neuraxial anaesthesia.Their high oestrogen levels influence cerebral vascular tone, increasing vascular distension in response to CSF hypotension. 6–7
b. Children: They are at greater risk of cerebrospinal fluid (CSF) leakage because their anatomy is much smaller. Consequently, the exact size and design of the needle remain critical determinants of risk in the paediatric population. 3–4
c. Elderly patients: Their risk is often underestimated, but they face greater vulnerability to severe neurological complications if Post-Dural Puncture Headache (PDPH) becomes chronic. Furthermore, age-related spinal deformities make needle insertion more challenging, increasing the number of puncture attempts. 4–6
d. Low Body Mass Index (BMI): A low Body Mass Index is independently associated with an increased risk of Post-Dural Puncture Headache (PDPH). This is due to reduced epidural pressure and a diminished natural plugging effect on cerebrospinal fluid (CSF) leakage into the epidural space. 4–6
Practice guidelines: Technique and decision-making support
Success in prevention lies in technique and in optimising the expertise of healthcare staff. Fewer puncture attempts directly equate to a lower risk of Post-Dural Puncture Headache (PDPH) and associated complications. 6–9
If it is strictly necessary to use a cutting needle, the bevel must always be aligned parallel to the longitudinal dural fibres (especially in obstetrics) so as not to sever them. 4-5-7
- If the patient is a young or pregnant woman → Always use a pencil-point needle as a first line of defence. 3
- If anatomical abnormalities are present (e.g. in the elderly) → Anticipate difficult access; minimise attempts by delegating the procedure to the most experienced operator. 6–9
Conclusion: A patient-centred approach
Post-Dural Puncture Headache (PDPH) is a largely preventable problem if the needle is selected appropriately and the puncture technique is refined. 3
Prioritizing pencil point tip needles over cutting tip needles in high-risk patients is not an absolute prohibition, but a vital risk-reduction strategy. 3
The clinical objective is to reduce morbidity, improve patient satisfaction and lower the costs associated with treatments such as epidural blood patch (EBP).8
“Choosing the needle is choosing patient safety”.
Bibliography
- “Atraumatic” Sprotte needle reduces the incidence of post-lumbar puncture headaches M. Strupp, MD, O. Schueler, MD, A. Straube, MD, S. Von Stuckrad–Barre, and T. Brandt, MD FRCP https://doi.org/10.1212/WNL.57.12.2310
- A randomised study to evaluate post-dural puncture headache following caesarean section: Comparison of median and paramedian approaches. M S Uluer, M Sargin, F Akin, E Uluer, O Sahin https://pubmed.ncbi.nlm.nih.gov/31719278/
- A study comparing 25 G Quincke and 25 G Whitacre spinal needles for post-dural puncture headache in the subarachnoid block. Shivrambhai D Prajapati, Bhargav R. Patel, Sachinkumar S. Patel, Ankit R Sorathiya, Dixitkumar B. Modh, Meetkumar Kansagra, Jaldeep Patel. https://impactfactor.org/PDF/IJPCR/15/IJPCR,Vol15,Issue7,Article5.pdf
- Prevention and Management of Post-Dural Puncture Headache (PDPH). Aynalem Befikadu, Sara Timerga, Fasil Mihretu, Fetene Siyoum and Amare Agmuas. https://clinmedjournals.org/articles/ijaa/international-journal-of-anesthetics-and-anesthesiology-ijaa-9-143.pdf?jid=ijaa
- Incidence and risk factors of post-dural puncture headache: prospective cohort study design. Bedilu Girma Weji, Mohammed Suleiman Obsa, Kidest Getu Melese & Gedion Asnake Azeze. https://link.springer.com/article/10.1186/s13741-020-00164-2
- Post-spinal puncture headache, an old problem and new concepts: review of articles on predisposing factors. Ali Jabbari, Ebrahim Alijanpour, Mehrafza Mir, Nadia Bani Hashem, Seyed Mozaffar Rabiea, Mohammad Ali Rupani. https://pubmed.ncbi.nlm.nih.gov/24009943/
- Post-dural puncture headache. Kyung-Hwa Kwak. https://pubmed.ncbi.nlm.nih.gov/28367283/
- The effect of spinal needle type on post-dural puncture headache in spinal anaesthesia: Prospective randomised study. Duygu Akyol, Mine Çelik, Necmiye Ay, Güneş Özlem Yıldız. https://pubmed.ncbi.nlm.nih.gov/39128075/
- Incidence and Factors Associated with Postspinal Headache in Obstetric Mothers Who Underwent Spinal Anaesthesia at a Tertiary Hospital in Western Uganda: A Prospective Cohort Study. Mohamud Jelle Osman, Joy Muhumuza, Yarine Fajardo, Andrew Kwikiriza, Baluku Asanairi, Rogers Kajabwangu, Marie Pascaline Sabine Ishimwe, Theoneste Hakizimana. https://pubmed.ncbi.nlm.nih.gov/37599669/




