Neonatal Peripherally Inserted Central Catheters (n-PICCs) are commonly used in Neonatal Intensive Care Units (NICUs) to administer vasoactive drugs and hyperosmotic solutions such as parenteral nutrition. These catheters are often maintained in place for 2 to 3 weeks and play a crucial role in neonatal care, particularly in cases where intravenous access is challenging. However, the choice of n-PICC insertion technique has significant implications for clinical outcomes, insertion success rates, and associated costs.
n-PICC Insertion Techniques
There are several traditional methods for inserting n-PICCs in newborns, with this study primarily focusing on the peelable cannula technique, referred to as SNT, and the Modified Seldinger Technique (MST).
- SNT: In the article we are referring to, SNT is used to denote the ‘Split Needle Technique’; however, based on the procedural details provided, the technique implemented corresponds to the Peelable Cannula Technique. This method uses an introducer composed of a puncture needle and a peelable cannula. It is a quick and relatively simple procedure; however, it can be associated with complications such as vein transfixion and increased difficulty in accessing small vessels due to the large size of the cannula (20 G).
- MST: This technique involves puncturing the vein with a very small-gauge needle (24 G), followed by the insertion of a guidewire, a dilator, and a peelable cannula before advancing the n-PICC (1 to 2 Fr). MST has demonstrated a higher success rate and requires fewer venipunctures, leading to better clinical outcomes.
MST: a clinical and economic choice
Several studies suggest that the implementation of the MST offers significant clinical benefits compared to the SNT, particularly by reducing the number of punctures required for successful catheter insertion. This decrease in the number of attempts leads to fewer complications, lowers the need for reinterventions, and results in less pain and stress for the patient.
The article addressing on the clinical relevance of the Modified Seldinger Technique provides further insights into MST’s clinical implications.
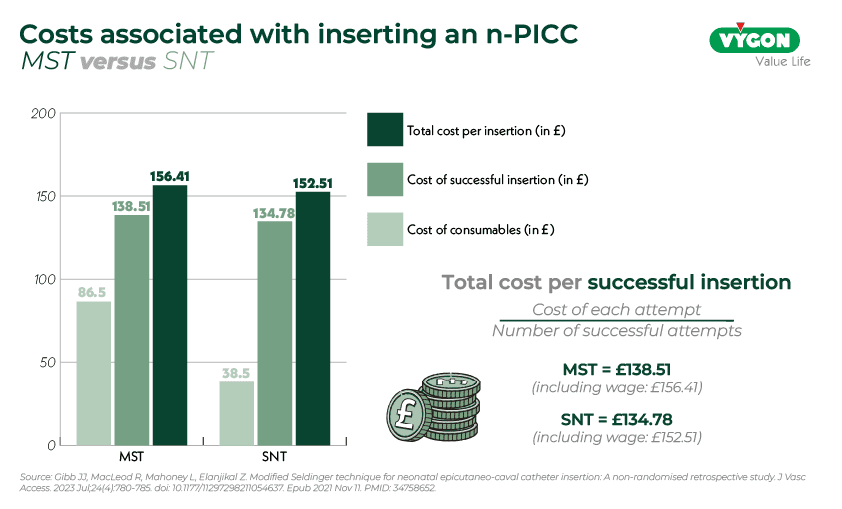
In this context, it is relevant to examine the economic impact of implementing this technique in clinical settings. A retrospective study conducted at St. Michael’s Hospital in Bristol, UK, compared the costs of MST and SNT for n-PICC insertion.
At first glance, the SNT technique appears to be less expensive than MST for both 1 Fr and 2 Fr catheters. This cost difference is primarily due to the use of less expensive consumables.
However, when a comprehensive economic analysis is performed, the picture becomes more nuanced.
Cost of consumables for an insertion attempt:
- For the MST technique, the cost was £86.50 for a 1 Fr catheter and £103.90 for a 2 Fr catheter.
- For the SNT technique, it was £38.50 for a 1 Fr catheter and £55.90 for a 2 Fr catheter.
Total cost per successful n-PICC catheter insertion:
- The cost was £138.51 for the MST technique and £134.78 for the SNT technique.
Total cost including the practitioner’s salary:
- When including the practitioner’s salary, the total cost per successful n-PICC was £156.41 for MST and £152.51 for SNT.
The economic analysis highlights a non-significant cost difference between the two insertion techniques. When both the costs of consumables and the salaries of the professionals performing the catheter insertion are taken into account, the total costs per successful inserted n-PICC are £156.41 for MST and £152.51 for SNT. Moreover, according to a study by Roland Van Rens, variations in staff salaries between institutions and countries can influence the cost-effectiveness evaluation of MST, potentially favoring this technique in long term. While MST involves a slightly higher initial expense for consumables, it significantly reduces the number of punctures required for successful insertion. This decrease in attempts provides indirect economic benefits, such as a lower risk of complications and reduced need for reinterventions, ultimately optimizing the overall procedural cost.
In this regard, the implementation of MST offers not only clinical advantages but also economic benefits.
Conclusion
In conclusion, although MST incurs a slightly higher cost when considering only consumables for an insertion, its significantly higher success rate compared to SNT compensates for this difference. Thus, when relating the cost to successful insertions, both techniques become comparable economically. Additionally, MST offers significant clinical advantages: by reducing the number of necessary venous punctures, it helps preserve venous capital, limit pain in newborns, and decrease the risk of complications associated with catheter placement. It constitutes a more effective approach in neonatology without incurring overall additional costs.
Would you like to learn more about the use of this technique in neonatology?
Bibliography
- Gibb JJC, MacLeod R, Mahoney L, Elanjikal Z. Modified Seldinger technique for neonatal epicutaneo-caval catheter insertion: A non-randomised retrospective study. J Vasc Access. 2021;1-6. doi:10.1177/11297298211054637
- Van Rens MFPT, Hugill K, van der Lee R, Francia ALV, van Loon FHJ, Bayoumi MAA. Comparing conventional and modified Seldinger techniques using a micro-insertion kit for PICC placement in neonates: a retrospective cohort study. Front Pediatr. 2024;Published May 2. doi:10.3389/fped.2024.1395395
A place to learn about health procedures and techniques from leading professionals.




