The incidence of mechanical complications during central venous catheter insertion is 6.2% to 11.8% for subclavian and internal jugular vein approaches, making it a challenge to select the ideal catheter length and avoid risks associated with the technique. 1
MECHANICAL COMPLICATIONS ASSOCIATED WITH CVC INSERTION
Failure to position the catheter tip correctly leads to different complications, some of them very serious:
- Cardiac tamponade. 1
- Cardiac perforation, vessel wall and cardiac erosions. 1
- Tricuspid valve damage. 1
- Malignant atrial damage. 1
- Ventricular arrhythmias. 1
- Pneumothorax. 1
- Haemothorax. 1
- Thrombus. 1
- Infection. 1
WHY DO THROMBI AND INFECTION OCCUR IN CENTRAL VENOUS CATHETER PLACEMENT?
When catheters are not inserted at an adequate depth they could easily find their way out of the superior vena cava, potentially increasing the risk of thrombus formation and/or infection. 1
WHY DOES VESSEL WALL PERFORATION AND CARDIAC PERFORATION OCCUR IN CENTRAL VENOUS CATHETER PLACEMENT?
Vessel wall and cardiac perforation may occur immediately during the procedure, due to a guide wire, dilator or catheter insertion. 1
But it can also occur late: as a consequence of catheter advancement with head, arm and trunk movement or tissue erosion caused by the catheter tip bounding against the vessel or cardiac wall, which is aggravated during cardiac contractions. 1
WHY DO ARRHYTHMIAS, VENTRICULAR TACHYCARDIA OR FIBRILLATION OCCUR DURING CENTRAL VENOUS CATHETER PLACEMENT?
Arrhythmias, including atrial and ventricular premature beats, ventricular tachycardia or fibrillation may occur when catheter insertion is excessive. These rhythm disturbances usually result from resistance to drug suppression and require catheter removal. 1
CATHETER LENGTH: RECOMMENDATIONS
There are different recommendations to reduce risks such as cardiac or vascular perforation, including omitting the bevelled or hard-tipped catheter, as well as avoiding the left-sided approach, which is associated with a higher risk of complications, or the immobilisation of the catheter. 1
However, the most effective method is to place the catheter tip extracardiac in the superior vena cava and confirm placement by chest X-ray. 1
WHERE SHOULD THE CATHETER TIP BE PLACED?
A central venous catheter is one whose tip is located in the proximal third of the superior vena cava, right atrium or inferior vena cava. These catheters can be inserted through a peripheral vein (PICC and FICC) or a proximal central vein (CICC), usually the basilic, femoral, internal jugular or subclavian vein.2
AREAS OF IMPORTANCE FOR THE PLACEMENT OF A CVC
Although discrepancies can be found between the different guidelines, what all recommendations agree on is that the correct position is between the lower third of the superior vena cava and the uppermost part of the right atrium, as this is where the greatest flow is found.
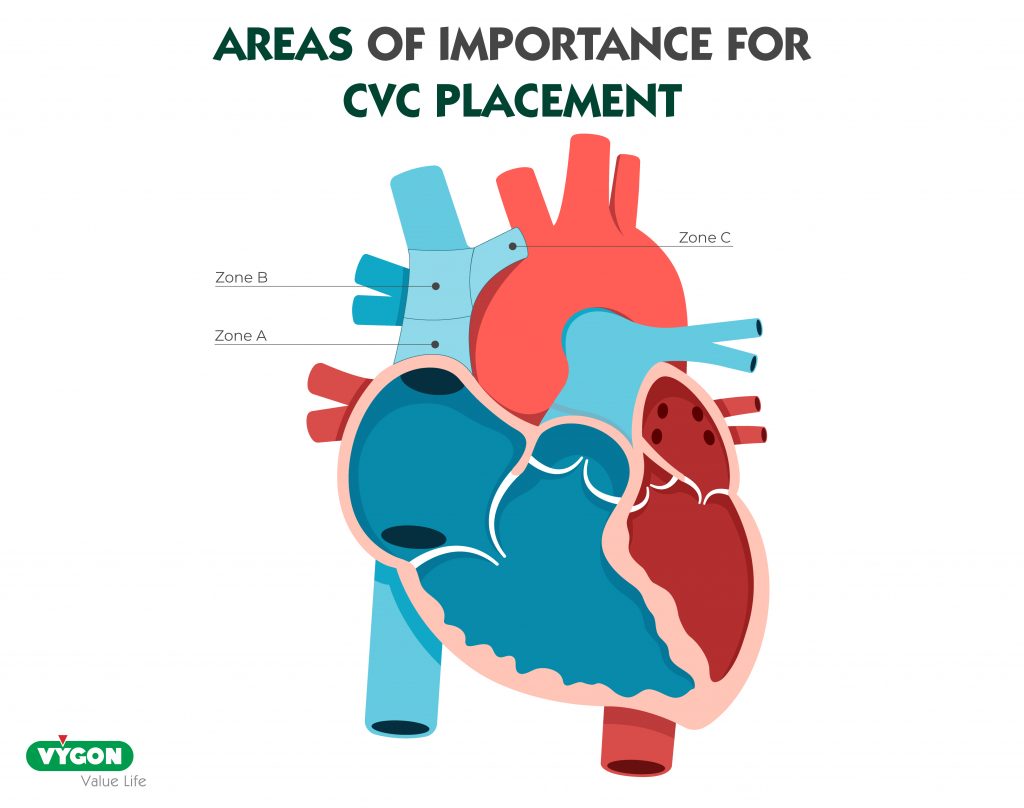
To place a catheter, the first thing to think about is where we want the tip of our catheter to be located. Some guidelines talk about three areas to which the catheter tip should be oriented: 1,10,11
- Zone A: represents the lower area of the superior vena cava and the upper area of the right atrium. In this zone, it is possible to place catheters parallel to the vessel from the left side. CVCs placed from the right side should ideally be moved back to zone B. 1,10,11
- Zone B: represents the area around the junction of the left and right innominate veins and the superior vena cava. This is an area suitable for catheters placed from the right side. Catheters placed from the left side will enter this area at a steep angle, increasing the risk of collision with the lateral wall of the superior vena cava. Therefore, ideally, they should be advanced towards zone A. 1,10,11
- Zone C: represents the left innominate vein proximal to the superior vena cava. This is a zone suitable for short-term fluid therapy and CVP monitoring, but not for inotropic infusions or long-term use. 1,10,11
ANATOMY RELEVANT TO CENTRAL VENOUS CANNULATION
In order to calculate the ideal length of our central venous catheter, it is essential to know the adjacent and adjacent structures to the selected access. Below are the most common central venous accesses: internal jugular vein and subclavian vein.
INTERNAL JUGULAR VEIN
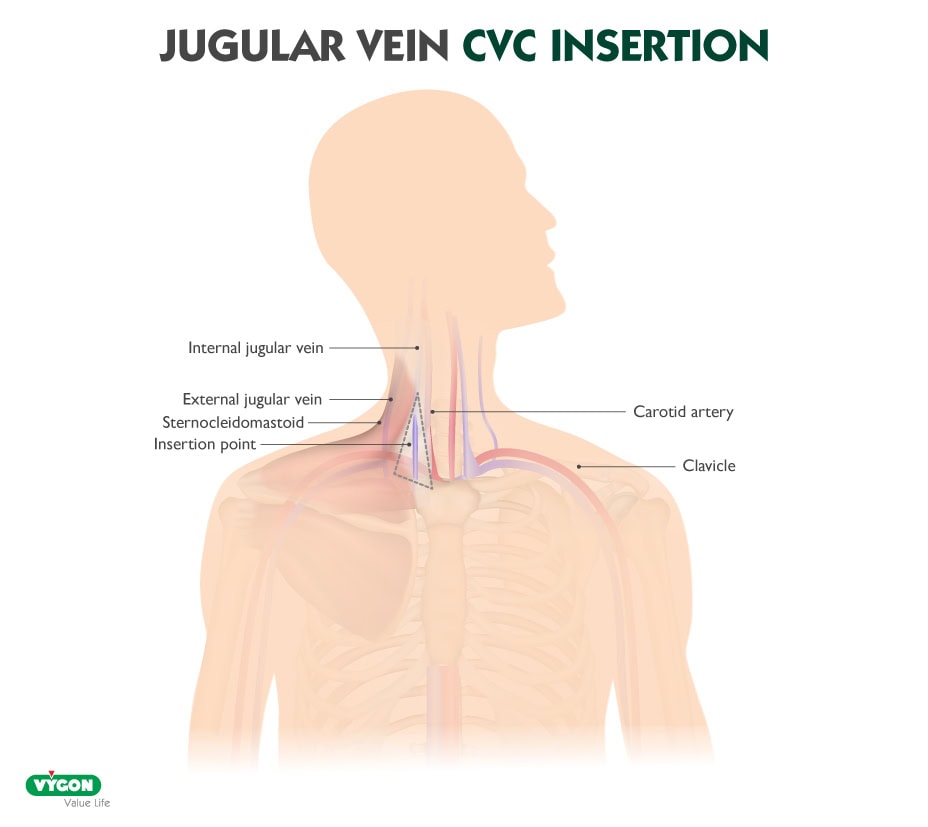
The essential surface anatomy is composed of the edges of Sedillot’s triangle: bordered by the clavicle inferiorly and by the sternal and clavicular heads of the sternocleidomastoid muscle medially and laterally.3,4
It is usually possible to palpate the carotid artery near the lateral side of the sternal head of the sternocleidomastoid. The internal jugular vein is usually superficial and lateral to the carotid artery. However, it should be noted that the positional relationship of the vessels will vary depending on the position of the head and neck. 3,4
In the awake supine patient, the edges of this triangle are accentuated by active elevation of the head. For the obese or uncooperative patient, the triangle is best defined by initial palpation of the trachea and then running the fingers laterally over the sternal head of the sternocleidomastoid towards the depression of the triangle. 3
The deep courses of the left and right internal jugular veins are not symmetrical. While the right internal jugular vein has a direct course under the superior vena cava, the left internal jugular vein courses to the right after joining the left subclavian vein to become the innominate vein, and the innominate vein subsequently courses downwards as it joins the superior vena cava. 3
The right internal jugular vein is usually preferred over the left for cannulation because of its larger diameter and because it allows a straighter path to the superior vena cava. 3
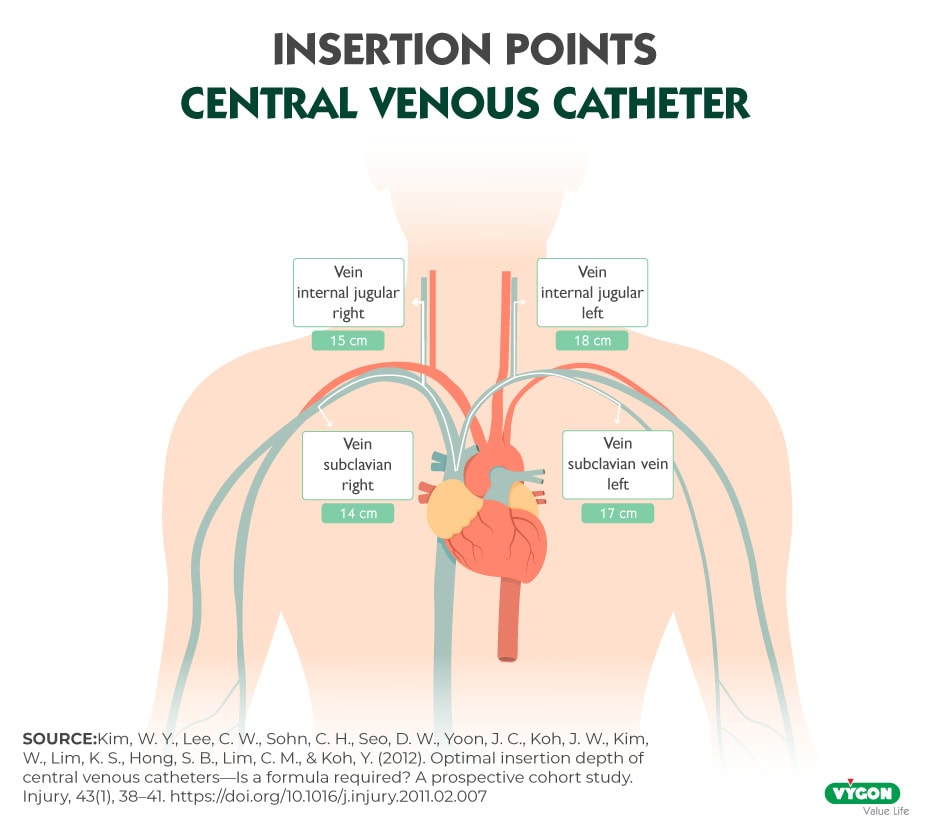
Length of catheter placed in internal jugular vein
In general, a measurement of 15 cm is recommended for the right internal jugular vein and 18 cm for the left internal jugular vein7. However, each patient is different, so it is important to take individual particularities into account. In addition, it is important to always perform the exploration and cannulation under ultrasound guidance, as this will allow us to avoid many risks and increase the success rate.
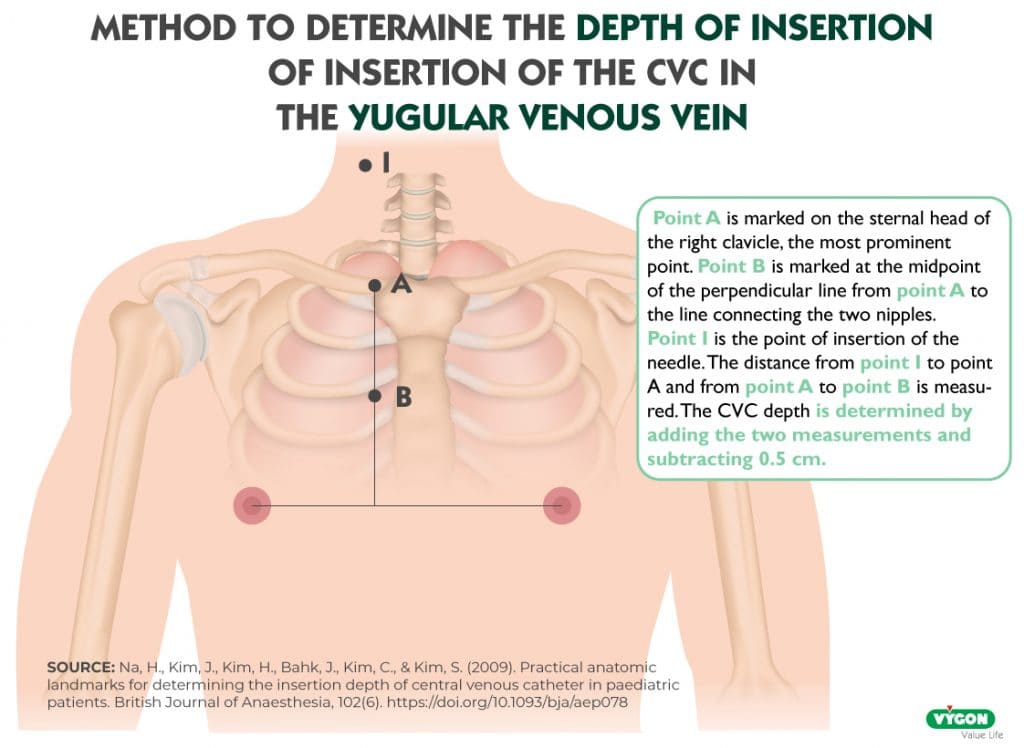
Another method is based on reference points, which can be seen in the illustration above. It consists of making a mark (point A) on the sternal head of the right clavicle, at the most prominent point of the clavicle. The next mark (point B) is made at the midpoint of the perpendicular line from point A to the line connecting the two nipples. The last mark is the point of insertion of the needle (point I). Adding the distance from point I to point A and from point A to point B and subtracting 0.5 cm gives the ideal catheter length for our patient.9
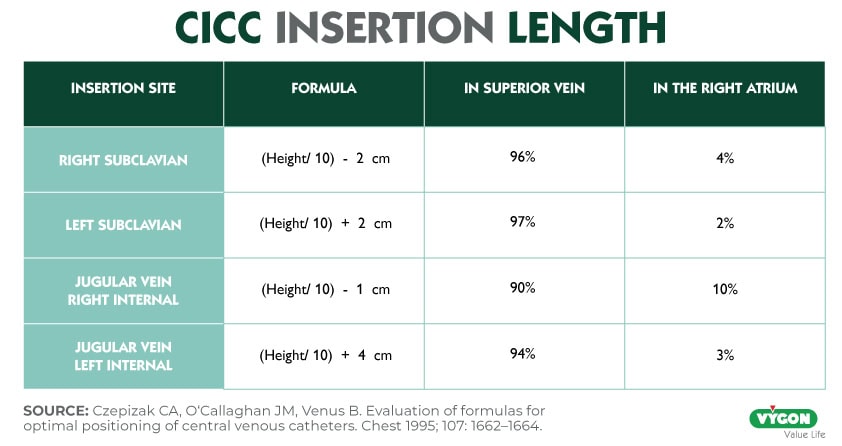
Finally, there are also formulas that can help us choose the ideal length of our catheter, in the case of the internal jugular vein8:
- Right internal jugular vein: (Height/10) – 1 cm
- Left internal jugular vein: (Height/10) + 4 cm
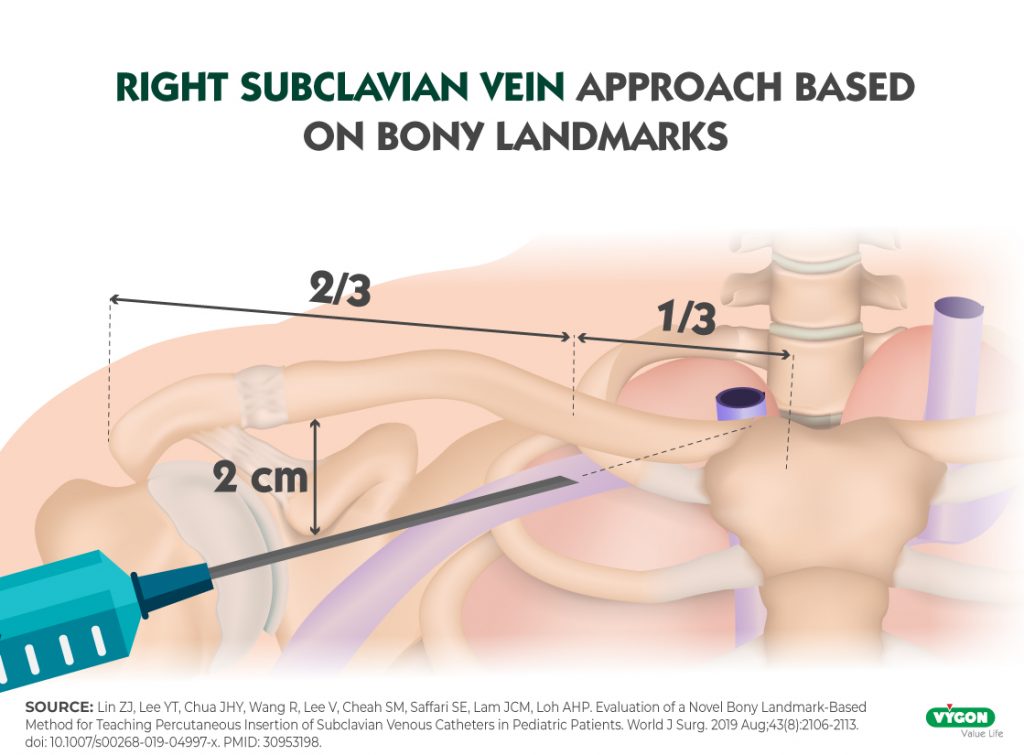
Subclavian vein
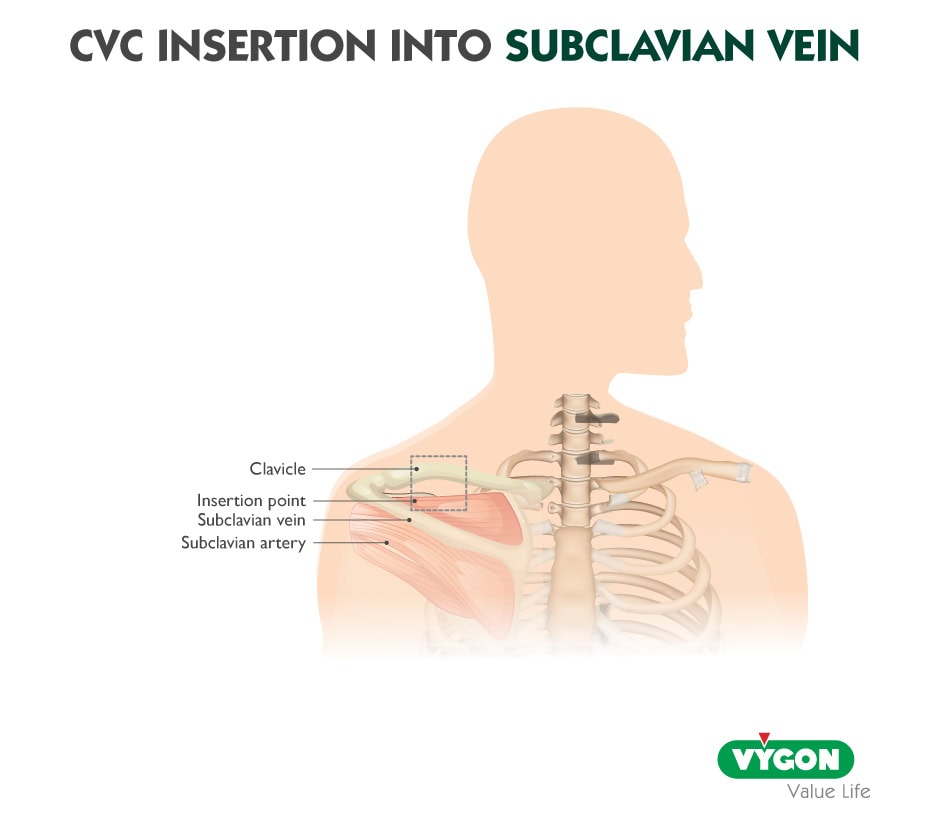
The aim of subclavian venipuncture is to pass the needle below the clavicle and above the first rib3. In order, from anterior to posterior, are: the clavicle, the subclavian vein, the anterior scalene muscle and the subclavian artery.5
The most common approach is infraclavicular, with two common insertion sites: 1 to 2 cm below the clavicle at the junction of its medial and middle thirds, or just below the clavicle at its midpoint5. Skin puncture at this point facilitates the passage of the needle under the clavicle, as a puncture closer to the clavicle creates difficulty in maneuvering the needle under the clavicle. 3
The subclavian vein is attached by fibrous tissue to the first rib and clavicle, which stabilises its position and diameter. 5
The patient should be placed in the Trendelenburg position to maximise venous filling and minimise the risk of air embolism. The position of the head and neck should be neutral. 3
Factors in the choice between right or left subclavian cannulation include the experience of the operator, but also5:
- Right subclavian cannulation avoids the thoracic duct and the right pleural apex is lower than the left. 5
- Left subclavian cannulation provides a direct route, less inclined to the superior vena cava, with less chance of misdirected catheterisation of the internal jugular vein. 5
As with the internal jugular veins, the deep courses of the right and left subclavian veins are not symmetrical. The venous course from the left subclavian vein arcs through the innominate vein to the superior vena cava in a smooth curve. In contrast, the right subclavian vein makes a steeper angled turn towards the superior vena cava, as it is joined by the internal jugular vein. 3
Length of catheter placed in subclavian vein
As with any other access, when choosing the ideal length of our catheter, we must take into account the differences that exist in each patient and make an accurate measurement. However, 14 cm is recommended for the right subclavian vein and 17 cm for the left subclavian vein.
Here we also find formulas that can help us to calculate the length of our catheter8:
- Right subclavian: (Height / 10) – 2 cm
- Left subclavian: (Height / 10) + 2 cm
ULTRASOUND MONITORING
Regardless of the access selected, it is important that cannulation is performed under ultrasound guidance because of the great benefits it brings.
Performing ultrasound-guided central venous access allows us to:
- Choose the optimal target vessel for a successful clinical outcome.
- Perform an examination prior to cannulation which allows us to determine associated complications or the presence of the healthy vessel prior to cannulation and its characteristics.
- Increase the success rate during vascular cannulation.
For all these reasons, today ultrasound-guided access is the standard of care for central venous access.
HOW TO PROPERLY SELECT THE LENGTH OF THE CVC?
The length of the CVC will depend on the vein to be cannulated and the clinical situation of the patient. There are no exact measurements that can be used for all patients due to the anatomical differences that can be found from one patient to another, however, as we have seen, studies have been carried out from which formulas have been extracted to help the professional select the most appropriate measurement for their patient based on their height.
However, it should be noted that these formulations do not take into account the likely differences in catheter insertion length due to variation in the same lateral approach, i.e. high internal jugular versus cricoid approaches or medial versus lateral subclavian approaches. 1
Another useful technique that does allow us to take into account the particularities of each patient is to measure based on reference points, which allows us to choose the most suitable length for each patient.
However, correct measurement is not always possible. In emergency situations, time is limited and the priority is to get central venous access as quickly as possible. When this is the case, there are a number of average measurements indicated for each insertion site. 1
BIBLIOGRAPHY
- Kujur, R., Rao, M. S., & Mrinal, M. (2009). How correct is the correct length for central venous catheter insertion. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine, 13(3), 159–162. https://doi.org/10.4103/0972-5229.58543
- Smith, R. N., & Nolan, J. P. (2013). Central venous catheters. BMJ. Published. https://doi.org/10.1136/bmj.f6570
- Bannon, M. P., Heller, S. F., & Rivera, M. (2011). Anatomic considerations for central venous cannulation. Risk management and healthcare policy, 4, 27–39. https://doi.org/10.2147/RMHP.S10383
- Ferrada, P. (2020b). Cómo hacer una canulación de la vena yugular interna. Manual MSD versión para profesionales. https://www.msdmanuals.com/es-es/professional/cuidados-cr%C3%ADticos/c%C3%B3mo-hacer-procedimientos-vasculares-centrales/c%C3%B3mo-hacer-una-canulaci%C3%B3n-de-la-vena-yugular-interna
- Ferrada, P. (2020). Cómo hacer la canulación de la vena subclavia infraclavicular. Manual MSD versión para profesionales. https://www.msdmanuals.com/es-es/professional/cuidados-cr%C3%ADticos/c%C3%B3mo-hacer-procedimientos-vasculares-centrales/c%C3%B3mo-hacer-la-canulaci%C3%B3n-de-la-vena-subclavia-infraclavicular
- Ibeas, J., Roca-Tey, R., Vallespín, J., Quereda, C., Crespo, R., Ochando, A., Cobo, J. L., & Grupo español multidisciplinar del acceso vascular (gemav). (2018). Guía clínica española del acceso vascular para hemodiálisis. Revista Oficial de la Sociedad Española de Enfermería Nefrológica, 21. https://www.revistaseden.org/files/Revistas_263_definitiva101310.pdf
- Kim WY, Lee CW, Sohn CH, Seo DW, Yoon JC, Koh JW, Kim W, Lim KS, Hong SB, Lim CM, Koh Y. Optimal insertion depth of central venous catheters–is a formula required? A prospective cohort study. Injury. 2012 Jan;43(1):38-41. doi: 10.1016/j.injury.2011.02.007. Epub 2011 Mar 5. PMID: 21377676
- Czepizak CA, O’Callaghan JM, Venus B. Evaluation of formulas for optimal positioning of central venous catheters. Chest. 1995 Jun;107(6):1662-4. doi: 10.1378/chest.107.6.1662. PMID: 7781364.
- Na HS, Kim JT, Kim HS, Bahk JH, Kim CS, Kim SD. Practical anatomic landmarks for determining the insertion depth of central venous catheter in paediatric patients. Br J Anaesth. 2009 Jun;102(6):820-3. doi: 10.1093/bja/aep078. Epub 2009 Apr 19. PMID: 19380312.
- Central venous access device insertion | Deranged Physiology. (2021). Deranged Physiology. https://derangedphysiology.com/main/required-reading/equipment-and-procedures/Chapter%20211/central-venous-access-device-insertion
- Safety Committee of Japanese Society of Anesthesiologists. Practical guide for safe central venous catheterization and management 2017. J Anesth 34, 167–186 (2020). https://doi.org/10.1007/s00540-019-02702-9
A place to learn about health procedures and techniques from leading professionals.




