Less Invasive Surfactant Administration (LISA) has transformed the respiratory care of preterm infants with respiratory distress syndrome (RDS). It offers a method of delivering life-saving surfactant while avoiding endotracheal intubation and the potential complications associated with mechanical ventilation.
As neonatal units across the UK adopt LISA, local experiences provide valuable insight into the practicalities, challenges, and successes of implementation. This article summarises real‑world learning from a neonatal unit that transitioned from traditional surfactant administration to routine use of LISA for spontaneously breathing preterm infants.
Why LISA?
Surfactant therapy is well established in the management of RDS. Traditionally, surfactant could only be administered via an endotracheal tube, requiring deliberate intubation and often mechanical ventilation — both of which carry known risks:
- ventilator‑induced lung injury
- volutrauma/barotrauma
- increased risk of chronic lung disease (CLD)
- need for sedation
- potential haemodynamic instability
LISA aims to reduce or avoid these complications by maintaining the infant’s own breathing effort and delivering surfactant through a thin catheter while the infant remains on continuous positive airway pressure (CPAP).
Key features of LISA include:
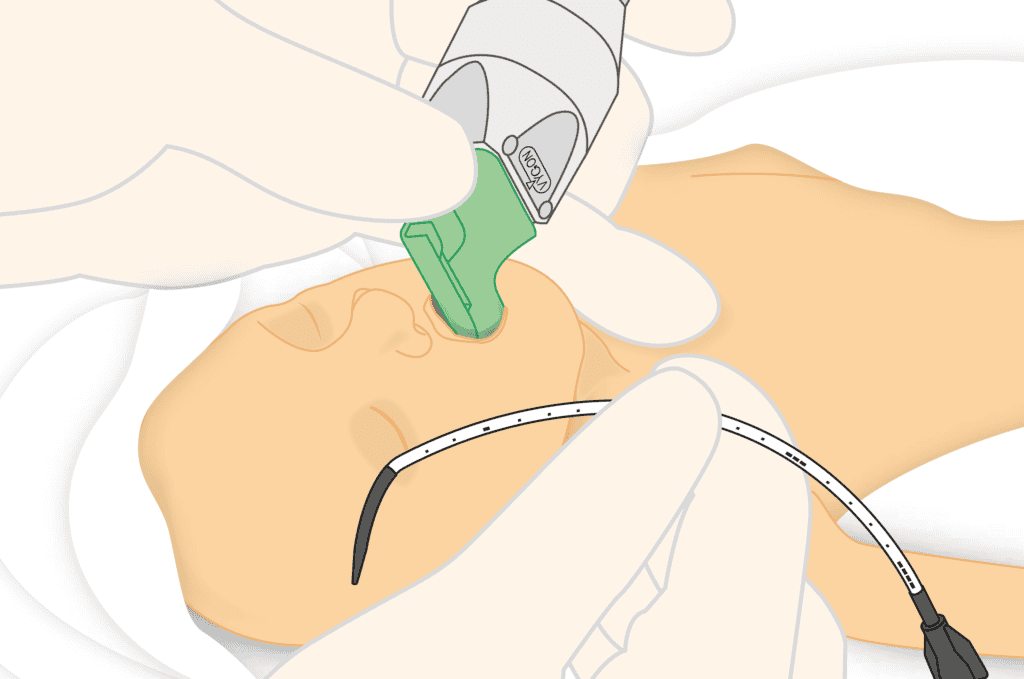
- Use of a fine, flexible catheter inserted under direct laryngoscopy
- No requirement for positive‑pressure ventilation
- Surfactant delivered in small aliquots while the infant continues to breathe spontaneously
- Rapid return to non‑invasive support after administration
This approach is designed to be physiologically gentle, minimising disruption to breathing patterns and reducing the risk of lung injury.
Implementing LISA: A Local Unit’s Approach
Background
The neonatal team at Ayrshire Maternity Unit had already developed strong pathways for early CPAP stabilisation and minimising invasive ventilation. However, they were keen to further reduce intubation rates for preterm infants with RDS. After reviewing published evidence and speaking with neighbouring centres, the team decided to introduce the LISA technique.
The goal was clear:
to deliver surfactant more gently, preserve spontaneous breathing, and strengthen the unit’s lung‑protective approach.
Training and Preparation
Before launching LISA, the Ayrshire team undertook:
- Structured training sessions for consultants, ANNPs, and senior nurses
- Hands‑on workshops focused on catheter placement and laryngoscopy technique
- Simulation-based practice, allowing staff to rehearse procedural flow
- Development of a local LISA guideline, outlining eligibility, preparation, documentation, and escalation criteria
By ensuring multidisciplinary ownership of the pathway, the unit aimed to create confidence and consistency from day one.
Early Implementation
In the first months, the team applied LISA to a small number of clinically appropriate infants—typically those:
- <32 weeks
- Stable on CPAP but showing increasing work of breathing
- Exhibiting FiO₂ requirements consistent with early surfactant need
Clinicians observed that infants generally tolerated the procedure well, with many maintaining spontaneous breaths throughout surfactant delivery.
Observed Benefits
Several positive trends emerged during the initial implementation phase:
1. Fewer intubations
The team saw a reduction in the number of infants requiring mechanical ventilation in the first 72 hours of life.
2. Improved respiratory stability
Infants who received LISA often stabilised on lower FiO₂ post‑procedure, with fewer episodes of desaturation.
3. Smoother transition back to non‑invasive support
Compared with traditional intubation‑surfactant delivery, babies typically resumed CPAP quickly and with less physiological disturbance.
4. Enhanced team confidence
Repeated practice and consistent protocol adherence helped staff feel increasingly comfortable with the technique.
5. Positive parental engagement
Parents appreciated that the approach was less invasive and aligned with gentle care principles. The team found that discussing LISA early in the neonatal journey helped reduce anxiety and strengthen communication.
Challenges and Lessons Learned
Like many units implementing LISA, Ayrshire Maternity Unit also noted key considerations:
- The technique requires good laryngoscopy skills, making experience a crucial factor.
- Establishing a clear threshold for surfactant administration helps ensure timely intervention.
- Team communication is essential, as LISA works best when roles and responsibilities are pre‑defined.
Over time, these insights were built into revised guidelines and onboarding materials to maintain high standards.
LISA in the Context of Modern Neonatal Care
The experience at Ayrshire Maternity Unit mirrors the growing trend across the UK towards minimally invasive respiratory support. LISA supports lung‑protective strategies and can help:
- Reduce chronic lung disease
- Minimise invasive procedures
- Improve long‑term respiratory outcomes
As more units adopt LISA, shared learning and consistent training will continue to drive success.
Conclusion
The LISA technique represents a significant advancement in the management of RDS, enabling surfactant administration while preserving spontaneous breathing and reducing the need for mechanical ventilation. The experience of neonatal teams such as those at Ayrshire Maternity Unit demonstrates how effective implementation can enhance outcomes, strengthen respiratory care pathways, and support gentler interventions for preterm infants.


