This is a summary of VYVAExperts2025. Watch in full here: https://learning.campusvygon.com/search?b=vyvaexperts
Early Challenges
Vascular access in oncology originally relied almost entirely on peripheral lines, beginning with steel, Teflon, and more recently, polyurethane. These caused frequent complications such as injury, extravasation and chemical phlebitis, placing significant burden on patients and nursing teams. Treatments were aggressive and required intensive monitoring, prompting the need for safer more effective options.
Each device involves not only complex clinical decisions, but also an emotional component, supported by nursing work that is often unnoticed but essential to ensuring continuity of treatment.
Introduction of Implantable Ports: A Major Breakthrough
The 1970s marked a turning point with the development of subcutaneous venous ports. Inspired by neurosurgical valve systems and arteriovenous shunts, the Port‑A‑Cath (1979) became widely adopted, transforming vascular access from an improvised necessity to a planned, strategic component of therapy.
Benefits included:
- Safer long‑term chemotherapy and parenteral nutrition
- Dramatically reduced extravasation risk
- More reliable central access for complex treatments
This shift introduced a new mindset of proactive device selection.
Hickman Catheters – Rise and Decline
Hickman catheters saw heavy use in the 1980s-1990s, especially in apheresis for the rescue of haematopoietic progenitor cells (e.g. breast cancer) and indicated for high‑dose chemotherapy. However, their use declined when evidence showed limited benefit from aggressive regimens. They remain valuable in select areas such as long‑term parenteral nutrition and dialysis and are valued for their longevity.
Transformation of Oncology Practice
The introduction of day hospitals marked a major organisational evolution in oncology services. These units enabled the delivery of high‑risk treatments without inpatient admission, allowing high-risk treatments to be administered in a safe and controlled environment while maintaining the patient’s independence. This represented an innovation and organisational adaptation for new and growing treatment regimes.
As treatment models evolved, nursing practice transformed alongside them. Nurses moved far beyond task‑based roles and became leaders in vascular access planning. Their responsibilities expanded significantly and now include:
- Shift from task‑based roles to clinical leadership
- Responsibility for assessment, indication, insertion and maintenance
- Prevention of technical and safety complications
- Continuous refinement of technique
This period also saw the birth of dedicated vascular access (VA) teams, which emerged directly in response to these growing clinical needs. These teams formalised specialist nursing expertise, ensuring consistency in practice, continuity of care, and a higher level of technical and clinical excellence.
The Rise of PICCs and Technological Advancements
Advances such as polyurethane catheter materials, ultrasound guidance and the modified Seldinger technique significantly improved the safety, durability and precision of PICC insertion, allowing placements to be more controlled and tailored to each patient’s needs and anatomy.
Standardised decision‑making tools like RaPeVA (Rapid Peripheral Vein Assessment) and RaCeVA (Rapid Central Vein Assessment) help ensure the most appropriate device is selected, supporting consistent practice across teams.
With these improvements, PICCs became central for intermediate‑term oncology treatments, reducing the need for repeated peripheral access. Meanwhile, PICC‑Ports offered the advantages of a fully implanted port; greater comfort, fewer dressing requirements and improved quality of life, but placed in the arm rather than the chest.
PICC-Ports bring practical benefits for patients by removing the need for weekly dressings, allowing water activities such as swimming, and reducing device visibility and stigma. Their safe use depends on expert nursing competence within vascular access teams. The presentation also highlights the professionalisation of nursing in this field, noting that this evolution empowers nurses and should be seen as an enhancement of care rather than intrusion.
When selecting and managing PICC-Ports, teams should monitor durability and resistance during prolonged use, watch for mechanical issues such as loops or fissures, consider how the device adapts to anatomical changes over time, and maintain vigilance for infection and thrombosis.
Today: Personalised, Patient‑Centred Vascular Access
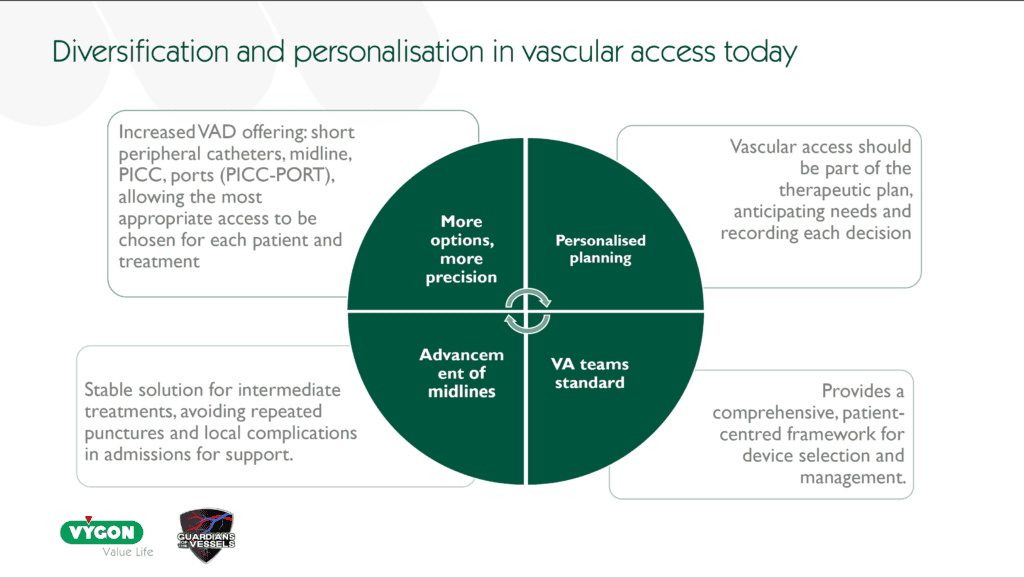
Cancer care is increasingly long term, and so requires tailored vascular access. These devices must support prolonged and combined treatments across the whole modern oncology pathway, not just chemotherapy. Vascular access teams should anticipate needs during critical phases such as prehabilitation and post radiotherapy complications. This involves selecting from a wide range of devices including peripheral cannulas, midlines, PICCs, ports and PICC-Ports to match the needs of each stage of treatment. Equity is essential so that every patient has access to the most suitable device for their life and clinical needs.
- Device choice is individualised and takes into account the patient’s therapy plan, anatomy and lifestyle so the access selected supports both safety and day to day living.
- In many centres, vascular access teams are now standard and provide the specialist expertise needed to guide assessment, indication, insertion and ongoing care.
- Excellence relies on training, experience and skilled use of ultrasound to ensure safe and precise insertion.
Throughout all decisions, patient quality of life remains central with modern devices reducing dressing requirements, minimising visibility and enabling activities such as swimming so patients can maintain a sense of normality during treatment.
Ongoing Challenges and Continuous Improvement
Ongoing challenges in vascular access highlight that even the best device requires meticulous and sustained aftercare. This depends on strong foundations such as clear protocols, regular audits, continuous training, and reliable traceability supported by meaningful safety indicators. These elements must sit within an organisational culture that understands and genuinely values modern vascular access, recognising its role in patient safety and treatment continuity. VYVAExperts2025 emphasises that vascular access devices are not merely technical tools but are bridges between clinical skill, patient trust and compassionate care, and that true quality comes from combining technical precision with a human centred approach.
A technically perfect insertion has limited value without aftercare that meets the same standard.
Safety, protocols and cultural change
Sustained safety depends on agreed protocols, regular audits, full traceability and meaningful safety indicators, underpinned by continuous training. The aim is to move from intuition to evidence-based care and to promote a culture where modern vascular access devices are known, used and respected across the organisation. Team strength comes from sharing practice, training together and driving improvement collectively.
Ultrasound is not enough
Although ultrasound guidance has transformed vascular access, simply having an ultrasound machine available is not sufficient. Excellence depends on extensive, specific training and even greater hands‑on experience, together with active learning from practitioners who lead clinical practice. True competence comes from judgement and consistency at the bedside, so placement and aftercare are delivered with precision and an understanding of subtleties that technology alone cannot replace.
Leadership, Coordination and Humanisation
Excellence is reinforced by nursing leadership and strong multidisciplinary coordination, supported by institutional recognition of vascular access expertise. Humanising the technique is central, turning technical skill into care that respects the person behind the device.
Conclusion
Vascular access devices are not just tubes and needles. They are bridges between clinical knowledge and patient hope, between science and everyday life, and between technique and trust. Turning technique into humanity is perhaps the best summary of everything we do.
Modern vascular access in oncology has evolved from a set of improvised peripheral lines to a sophisticated, patient‑centred system led by expert nursing teams using evidence‑based protocols and advanced technologies.