Vascular access is the most common procedure that patients in tertiary care undergo and, with recent improvements and advances in technology, the choices of devices and insertion techniques have evolved. It is therefore important that education and training is available to assist practitioners in this field1.
Central Venous Catheters (CVCs) are tools in modern healthcare, enabling the administration of medications, fluids, and nutrition, as well as facilitating haemodynamic monitoring. While central venous catheters have been used in clinical practice for decades, their role within vascular access is evolving rather than expanding. The use of acute CVCs is generally not increasing; in fact, some organisations now favour PICCs and midlines as safer alternatives for medium‑term therapy. However, CVCs remain essential in critical care, haemodynamic monitoring, rapid resuscitation, and situations where peripheral or midline access is not suitable.
This article explores the responsibilities of healthcare professionals, the anatomical and physiological considerations for CVC placement, and the criteria for selecting the appropriate device.
Evolving Roles of Nurses and Advanced Healthcare Practitioners (AHPs)
Over recent decades, the responsibilities of nurses and allied health professionals have expanded in response to healthcare system reforms, workforce shortages, and technological advancements. This shift has been driven in part by Working Time Regulation initiatives such as the European Working Time Directive2 and Modernising Medical Careers3.
In response to these changes in professional boundaries, Critical Care and ICU Nurses and AHPs now play a pivotal role in inserting CVCs under local competency, governance, and medical oversight, with no external training support. This is also due to additional factors including an ageing population, increased consumer expectations, technological advances, and growth in radiological procedures. Their involvement not only enhances service efficiency but also improves patient outcomes by ensuring timely and skilled catheter placement.
Legal and Ethical Responsibilities
With expanded roles come increased legal and ethical responsibilities. Nurses are accountable to the Nursing and Midwifery Council (NMC)4, while AHPs are governed by the Health and Care Professions Council (HCPC)5. Both regulatory bodies emphasise the importance of maintaining up-to-date knowledge and skills, particularly when undertaking advanced procedures such as CVC insertion.
Venous Anatomy and Physiology
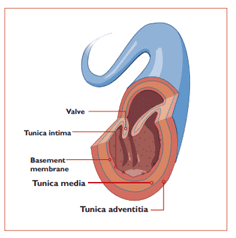
A thorough understanding of venous anatomy is essential for safe and effective CVC placement. Veins are composed of three layers: the tunica intima (inner), tunica media (middle), and tunica adventitia (outer). The integrity of the tunica intima is particularly important, as trauma can lead to thrombosis and other complications6.
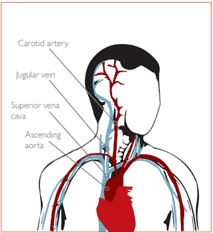
CVCs are typically placed in central veins such as the superior vena cava (SVC), inferior vena cava (IVC), or right atrium. Access is usually gained via peripheral veins like the internal jugular, subclavian, or femoral veins, using the Seldinger technique for correct placement. Correct tip placement, ideally in the lower third of the SVC or upper right atrium is crucial to minimise risks such as thrombosis, cardiac tamponade, and catheter malfunction7,8,9. Understanding this anatomy is critical in preventing complications such as malposition, venous injury, or arrhythmia during CVC placement.
Types of CVCs and Selection Criteria
CVCs vary in design, material, and functionality. Selection should always be tailored to the clinical indication, expected duration of therapy, and individual patient factors. Different catheter types offer distinct advantages in specific situations.
Common types of CVCs include:
Polyurethane catheters for short-term access.
Polyurethane provides a good balance of strength and flexibility making it suitable for acute settings such as critical illness, perioperative care, or short inpatient stays where high flow rates are required. They are generally preferred when rapid infusion, vasopressor administration, or frequent blood sampling is expected.
Antimicrobial catheters with silver ion technology.
These are selected when the patient has an increased risk of infection such as in intensive care units or oncology patients with prolonged neutropenia. Silver ion coatings help inhibit microbial colonisation at the insertion site and intra-luminally, lowering the incidence of catheter-related blood stream infections, and without risk of chlorhexidine allergy or anaphylaxis.
Antibiotic-impregnated catheters for high-risk patients10.
These are typically used in high-risk patients, for example, those with repeated line infections, those requiring long dwell times, or when the consequences of infection would be severe. They may provide additional protection in environments with high catheter use or limited line replacement opportunities.
Rationale for Selecting Specific Catheter Features:
Number of lumens: Based on the need for multiple infusions.
Choosing the correct number of lumens at the start of treatment is essential.
Multi-lumen CVCs allow simultaneous delivery of incompatible medications, blood products, parenteral nutrition, and high‑flow infusions.
Using a multi-lumen catheter from the outset reduces the need for adding extra lines later, which decreases cumulative insertion risks such as bleeding, infection, and mechanical complication.
Starting with a single‑lumen catheter and later adding additional access points increases patient discomfort, requires more staff time, and exposes the patient to further procedural risk.
A three‑lumen CVC is commonly selected in critical care because it provides sufficient versatility without compromising line diameter for high‑flow infusions.
A five-lumen high-flow CVC is also a consideration to avoid the need for the use of multiple insertion sites (Read more about five lumen high-flow CVCs: Why Use 2 when One Will Do)
Length: Determined by insertion site and patient anatomy11.
The ideal length depends on the insertion site and patient anatomy.
- Shorter catheters are suitable for internal jugular or subclavian insertion where the path to the superior vena cava is short.
- Longer catheters may be required for femoral access or in taller patients to ensure the tip reaches the correct central position. Optimal tip placement reduces the risk of thrombosis, arrhythmia, and malposition.
Material and coating: To reduce infection risk and improve biocompatibility12.
Material choice can influence complication rates.
- Polyurethane offers durability and kink resistance.
- Silicone is more flexible and biocompatible, often used for long‑term devices but less ideal for high‑pressure infusions.
- Antimicrobial or hydrophobic surface coatings reduce bacterial adhesion and biofilm formation, which is particularly beneficial for patients requiring long‑term CVC support.
Contraindications and operator considerations13
Contraindications such as coagulopathy, local infection at the intended insertion site, or thrombosis must be assessed prior to placement. The experience of the operator also strongly influences safety and success. Skilled placement minimises complications like arterial puncture, malposition, and pneumothorax, while also improving first‑pass success rates and overall patient comfort.
Conclusion
The landscape of CVC use is evolving, with nurses and AHPs taking on increasingly complex roles in their placement and management. Understanding the legal framework, anatomical considerations, and device options is essential for delivering safe, effective care. With appropriate training and adherence to best practice guidelines, healthcare professionals can ensure optimal outcomes for patients requiring central venous access.
Clinicians must work within the scope of their professional registration. Doctors are accountable to the General Medical Council (GMC), nurses to the or the Nursing and Midwifery Council (NMC), and advanced healthcare practitioners to the Health and Care Professions Council (HCPC), and should be familiar with their relevant guidelines and developments. Specific competency levels required for CVC insertion are listed in the Anaesthetic and ICM Curricula (ROCA). Use of Vascular Access Devices can result in harm to patients and negative outcomes. Vygon (UK) Ltd accepts no liability for the content of this series or the consequences of any actions taken on the basis of the information provided.
Continue Reading
- Article 1: Understanding CVCs: Roles, Anatomy, and Device Selection

- Article 2: Preparing for CVC Insertion – Patient Assessment, Consent, and Pain Management

- Article 3: Infection Prevention and Aseptic Techniques

- Article 4: Foundations of Ultrasound Physics and Applications

- Article 5: Central Venous Lines – Insertion Techniques and Pain Management

- Article 6: Navigating Complications in Central Venous Access

- Article 7: Post-Insertion Care, Maintenance and Safe Removal

References
1. Moureau N, Lamperti M, Kelly LJ, et al. Evidence-based consensus on the insertion of central venous devices. Br J Anaesth. 2013;110:347–56.
2. Health and Safety Executive. Working Time Regulations (1998).
3. Department of Health. Modernising Medical Careers (2006).
4. Nursing and Midwifery Council (NMC). The Code: Professional Standards of Practice and Behaviour for Nurses and Midwives. 2015.
5. Health and Care Professions Council. Standards of Conduct, Performance and Ethics. 2016.
6. Tortora GJ, Derrickson BH. Principles of Anatomy and Physiology. 14th ed. Wiley; 2014.
7. Bodenham A, et al. Safe vascular access guidelines. Anaesthesia. 2016.
8. Warakaulle DR, Phillip-Hughes J. In: Hamilton H, Bodenham AR. Central Venous Catheters. Wiley-Blackwell; 2009.
9. Gee A. The importance of ideal central venous access device tip position. Br J Nurs. 2012;21(21):S19–24.
10. Loveday HP, et al. epic3: National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections. J Hosp Infect. 2014.
11. Bodenham A, et al. Anaesthesia. 2016.
12. Maki DG, Ringer M, Alvarado CJ. Prospective randomised trial of antiseptics for catheter insertion. Lancet. 1991;338:339–43.
13. Dougherty L, Lamb J. IV Therapy in Nursing Practice. 2nd ed. Blackwell Publishing; 2008.