Effective fluid management is a cornerstone of safe anaesthesia, perioperative care, and critical care medicine. Yet, even with decades of clinical experience, determining the right amount of fluid for each patient remains one of the most debated aspects of haemodynamic management.
Traditional indicators (heart rate, blood pressure, urine output) offer useful information, but none reliably predicts whether a patient will benefit from further intravenous fluids. As a result, clinicians may over‑ or under‑prescribe fluids, risking complications such as pulmonary oedema, tissue oedema, delayed recovery, or organ hypoperfusion.
Cardiac output (CO) monitoring changes this picture.
By providing real‑time, objective haemodynamic data, CO monitoring allows clinicians to base fluid management on measurable physiological responses rather than intuition alone. The result is a more precise, personalised, and evidence‑driven approach to patient care.
The Role of Cardiac Output Monitoring in Modern Fluid Therapy
1. Understanding True Circulatory Status
Blood pressure alone cannot reliably indicate whether cardiac output is adequate. A patient may be hypotensive due to low vascular tone, not low blood volume, and giving fluids in this context may be ineffective or even harmful.
CO monitoring provides a fuller picture by measuring parameters such as:
- Cardiac Output (CO) – overall circulatory performance
- Stroke Volume (SV) – the volume ejected per heartbeat
- Dynamic preload indicators (e.g. SVV, PPV – depending on monitoring technology)
- Systemic Vascular Resistance (SVR) – vascular tone and afterload
This multidimensional view helps clinicians differentiate between causes of instability and choose the most appropriate therapy.
2. Predicting Fluid Responsiveness Before Giving a Bolus
One of the most important contributions of CO monitoring is the ability to test fluid responsiveness. Evidence shows that only about half of haemodynamically unstable patients will actually respond positively to fluids.
CO monitoring enables dynamic, physiologically meaningful assessments such as:
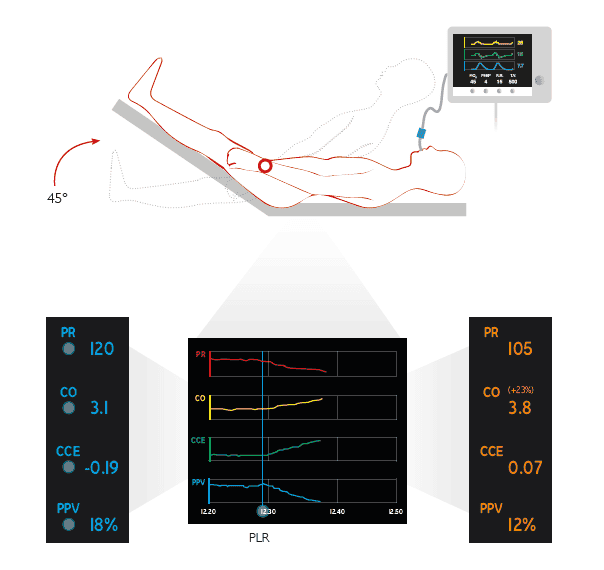
Passive Leg Raise (PLR)
A reversible manoeuvre that simulates a fluid bolus by temporarily increasing venous return.
A significant rise in stroke volume indicates the patient will benefit from fluids.
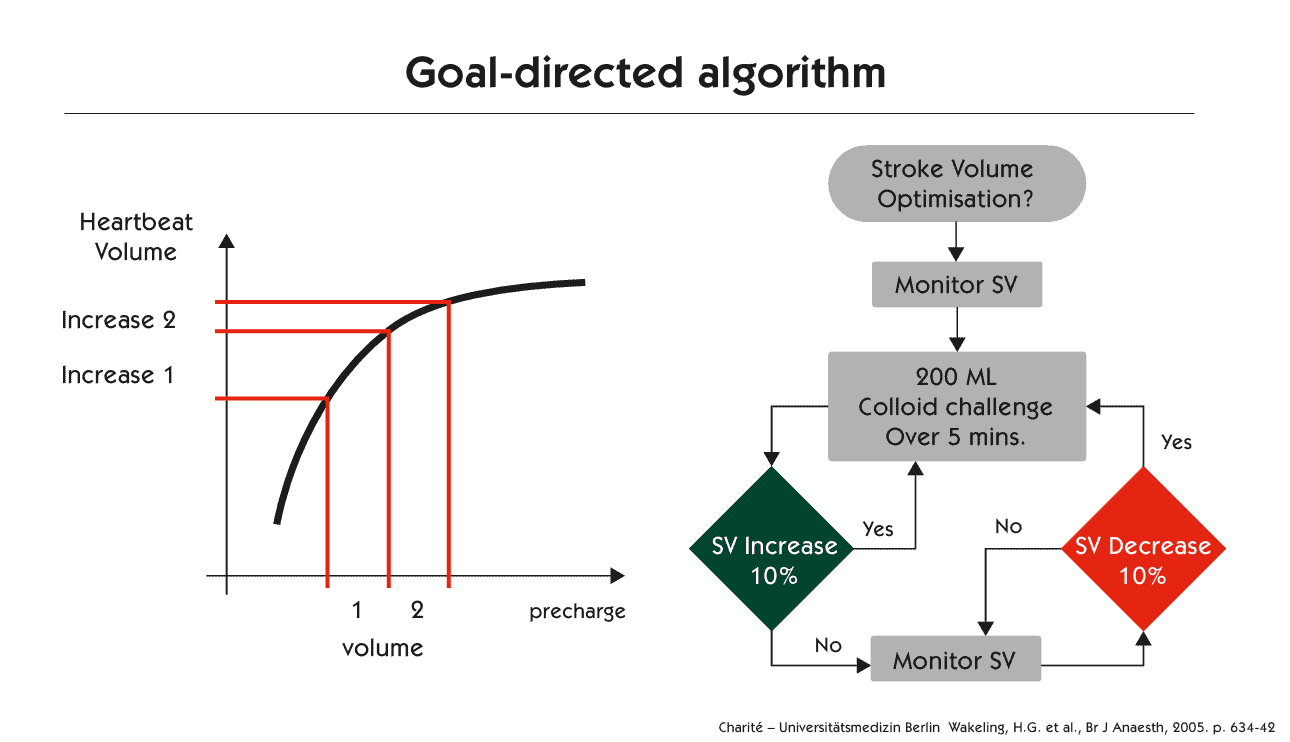
Mini or Standardised Fluid Challenges
Administering a small bolus (e.g. 250 mL) while observing changes in real‑time CO or SV.
If stroke volume increases by a clinically relevant threshold (often ≥10%), the patient is fluid responsive.
Dynamic Indices
Certain technologies can measure SVV or PPV to identify whether a patient is preload dependent.
The advantage:
Fluids are no longer given “just in case”, they are given only if they are likely to improve cardiac output and tissue perfusion.
3. Guiding Optimisation and Stopping Fluid at the Right Time
Once a patient is confirmed as fluid responsive, CO monitoring supports ongoing optimisation:
- Fluids are administered in small increments while continuously observing SV and CO.
- When increases plateau, the clinician knows the patient has reached an optimal preload.
- This allows confident, evidence‑based decisions to stop fluid administration.
Avoiding unnecessary fluid loading reduces risks such as:
- Pulmonary oedema
- Interstitial oedema
- Delayed wound healing
- Longer ICU or hospital stays
When fluid optimisation is complete, but instability remains, clinicians can move logically to the next step (e.g. vasopressors or inotropes), supported by objective measurements rather than clinical uncertainty.
4. Supporting Enhanced Recovery and Clinical Efficiency
Evidence‑based, CO‑guided fluid management aligns with enhanced recovery principles by promoting:
- Better tissue perfusion
- Reduced complications
- Shorter postoperative and ICU stays
- More predictable recovery trajectories
For busy clinical teams, it also improves communication and reduces ambiguity – CO data provides a shared, objective language for assessing haemodynamic status and planning interventions.
Why Evidence-Based Fluid Management Matters
Fluids are among the most common interventions in perioperative and critical care, yet also one of the most variable. Under‑resuscitation puts organs at risk; over‑resuscitation contributes to morbidity.
Cardiac output monitoring enables clinicians to identify an individualised therapeutic range that aligns with each patient’s physiological status and is guided by real‑time hemodynamic data.
Conclusion
Cardiac output monitoring is not just a device – it is an approach to patient care that reduces uncertainty, enhances safety, and supports better outcomes. By integrating CO monitoring into routine practice, clinicians can:
✔ Gain a complete, dynamic understanding of haemodynamic status
✔ Predict who will benefit from fluids before giving them
✔ Optimise perfusion while avoiding fluid overload
✔ Support a more structured, evidence‑based approach to resuscitation
In an environment where precision matters, CO monitoring gives clinicians the clarity they need to deliver the right therapy, at the right time, for the right patient.


