The safe and effective insertion of a central venous catheter (CVC) requires a solid understanding of both the theoretical and practical aspects of the procedure. This includes a foundational knowledge of ultrasound physics and the ability to apply ultrasound guidance accurately during catheter placement. Clinicians must also demonstrate the competence and confidence to perform the insertion itself, while ensuring appropriate post-procedure care and thorough documentation. Together, these elements support high standards of patient safety and clinical practice.
An Introduction to Ultrasound
An early meta-analysis concluded that ultrasound guidance significantly reduced placement failures[1]. In addition, the analysis showed a decrease in complications. Alternative meta-analysis provided evidence which supported the use of two-dimensional ultrasonography for central venous catheter placement[2]. More recently, similar results demonstrated both an increased first puncture rate in addition to an increased successful catheter insertion[3],[4].
From these few studies it could be suggested that the evidence to use ultrasound guidance is compelling. However, we have to be aware that, when introducing new technologies, there is always a learning curve and during this time complication rates can increase[5].
Ultrasound training is now recommended as part of CVC placement training[6],[7]. In addition to simulation training a good knowledge of the physics of ultrasound and how this relates to image production and interpretation is deemed necessary[8].
The National Institute for Clinical Excellence (NICE) further reiterates this by stating, “The use of two-dimensional (2-D) imaging ultrasound guidance should be considered in most clinical circumstances where CVC insertion is necessary either electively or in an emergency situation”[9].
As the use of ultrasound guidance to place central venous catheters requires a competent and experienced operator[10], training for all nurse specialists is paramount.
Current guidelines state: “It is recommended that all those involved in placing CVCs using two-dimensional (2-D) imaging ultrasound guidance, should undertake appropriate training to achieve competence”[11].
Basic Ultrasound Physics
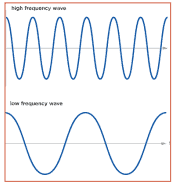
Ultrasound is sound energy in the form of waves that have a frequency above the range of human hearing. The human ear can detect up to approximately 20,000 cycles per second (20,000Hz), at this point sonic range ends and the ultrasonic range begins.
Ultrasound is used to locate objects by similar means echolocation used by bats, whales and dolphins as well as sonar used by submarines.
In ultrasound medical imaging, the following occurs:
- High frequency sound waves from the machine are transmitted through a medium into the body via a transducer
- As the sound waves travel into the body, they hit structures (boundaries) such as fluid, soft tissue or bone
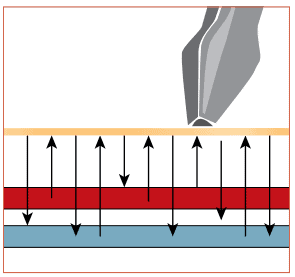
- Some of the sound waves are reflected back to the transducer while some travel on further until they reach another boundary and at this point, they are reflected back
- Reflected waves are picked up by the probe and relayed back to the machine
- By using the speed of sound in tissues, the machine is able to calculate the distance from the probe to the tissue or organ (boundaries) and the time of each echo’s return
- The two-dimensional image displayed on the machine reflects the distance and intensities of the echoes
- All of the above occur simultaneously in real time scanning.
Transducer (Probe)
The probe transmits and receives the ultrasound beam on contact with the patient’s skin. It takes a thin slice of the object being imaged. Rotate or angle to change views. It is important to note that the length of the transducer face is only 1mm thick. The length of the beam is dependent upon the selected depth. The markings on the transducer provide a guide to the orientation.
When performing an ultrasound guided puncture, the needle must remain in the ultrasound beam to ensure it is visible on the screen at all times.
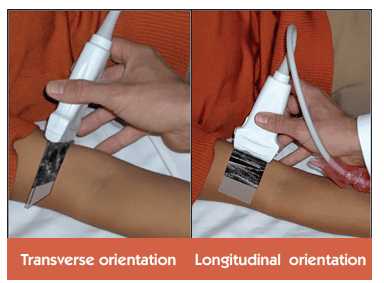
Orientation
Most ultrasound machines have markers to allow correct orientation. This may be in the form of a groove on the side of the transducer. This groove teams up with an orientation maker on the ultrasound screen. If orientation is incorrect, this can lead to confusion as when the probe is moved to the left, the image will move to the right. Therefore, correct orientation is important.
Another simple way to ensure correct orientation is to touch the side of the transducer with your finger. On the screen a flicker will appear which indicates the orientation of the transducer.
Transverse
In transverse orientation the vessel will appear round. If a puncture is performed in the centre of the probe, this will lead to a puncture in the centre of the vessel.
Longitudinal
A longitudinal orientation will display the vessel as a line. Puncturing at this angle will allow the guidewire to be followed some way along the vessel.
Frequency
It is important to use the highest frequency transducer that will reach the depth required. In vascular access the vessel depth is usually relatively superficial, so a high frequency probe will result in less depth, whereas a low frequency probe will result in more depth.
Blood Vessel Characteristics on Ultrasound
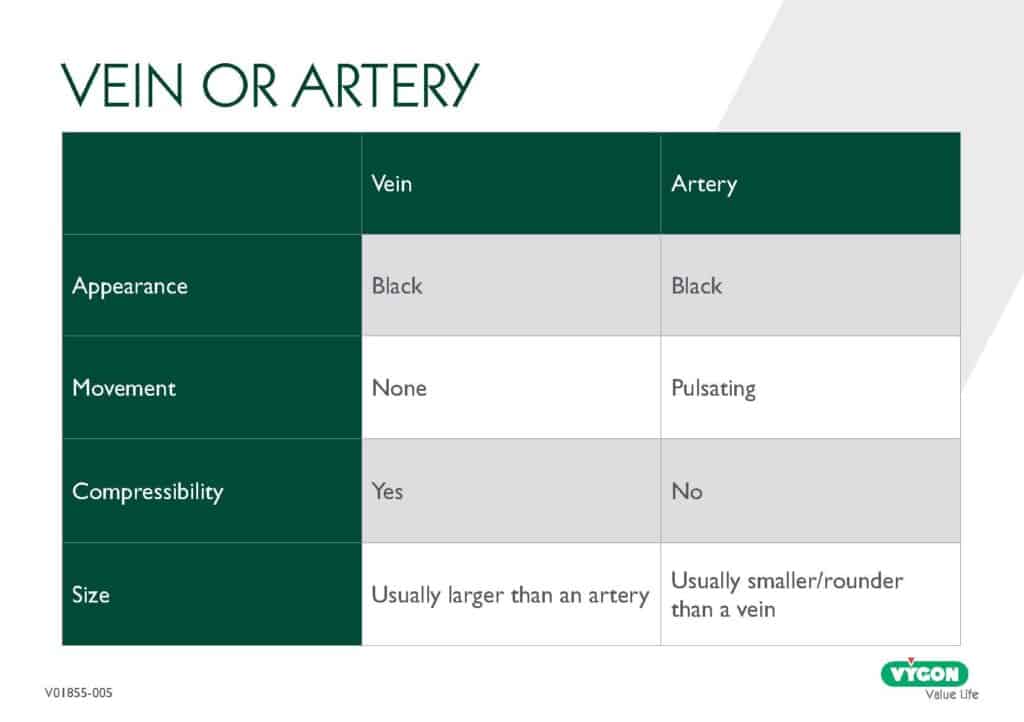
As well as allowing visualisation of the vessels, ultrasound can confirm patency of the vessel. A thrombosed vessel will not compress. In addition, the vessel will appear white instead of black on the screen.
Gain
This control improves the vision on the screen. It is similar to a brightness control and should be used to enhance the appearance prior to puncture. This control can be near gain, which will change the appearance at the top of the screen. Far gain will adjust the appearance at the bottom of the screen and, finally, there will be the option of changing the overall gain of the whole screen.
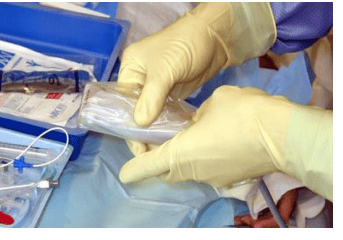
Probe Preparation
One of the most important pre-scanning aspects is the preparation of the probe. Ultrasound requires a couplant to allow waves to transmit. Ultrasound gel needs to be placed within the ultrasound probe sheath cover as well as to the skin surface to ensure optimal visualisation. Air within the sheath cover will lead to a poor view, which may reduce puncture success rate. This procedure may require two people, one who is scrubbed whilst the other would not be. It is important to ensure air free coupling between all surfaces.
Some Common Mistakes When First Using Ultrasound
- Watching your hands instead of the screen
- Holding the ultrasound probe incorrectly
- Collapsing the vein with probe pressure
- Puncturing at the wrong angle.
Conclusion
Ultrasound guided puncture can be a hugely beneficial skill which enhances both the safety and accuracy of vascular access procedures, including CVC insertion. Following best practices can significantly improve outcomes and puncture success rates and reduce complications discussed in earlier articles, such as obliteration of the vessel. Using the advice set out above, outlining key steps and considerations for practitioners to develop confidence and competence in using ultrasound for guided puncture.
Continue Reading
- Article 1: Understanding CVCs: Roles, Anatomy, and Device Selection

- Article 2: Preparing for CVC Insertion – Patient Assessment, Consent, and Pain Management

- Article 3: Infection Prevention and Aseptic Techniques

- Article 4: Foundations of Ultrasound Physics and Applications

- Article 5: Central Venous Lines – Insertion Techniques and Pain Management

- Article 6: Navigating Complications in Central Venous Access

- Article 7: Post-Insertion Care, Maintenance and Safe Removal

References
[1] Randolph, A.G. Cook, D.J. Gonzales, C.A. Pribble, C.G. (1996) Ultrasound guidance for central venous catheter placement. – A meta – analysis of the literature. Critical Care Medicine: 24 (12) 2053 – 2058
[2] Hind, D. Calvert, N. McWilliams, R. Davidson, A. Beverley, C. Thomas, S. (2003) Ultrasonic locating devices for central venous cannulation: Meta analysis. British Medical Journal. 327 (7411) 361
[3] Dodge, K.L. Lynch, C.A. Moore, C.L. Biroscak, B.J. Evans, L.V (2012) Use of Ultrasound Guidance Improves central venous catheter insertion success rates among junior residents. Journal of Ultrasound Medicine. 31 (10) 1519 – 1526
[4] Warrington, WG. Penoyer, DA. Kamps, TK et al. (2012) Outcomes of Using a Modified Seldinger Technique for Long Term Intravenous Therapy in Hospitalized Patients with Difficult Venous Access. Association of Vascular Access. 17 (1) 24 – 30
[5] Bold, R.J. Winchester, D.J. Madary, A.R. Gregurich, M.A. Mansfield, P.F. (1998) Prospective, randomised trial of Dopplar – assisted Subclavian vein catheterisation. Achieves of Surgery. 133(10) 1089 – 1093
[6] Moureau, N. Lamperti, M. Kelly, LJ et al. (2013) Evidence – based consensus on the insertion of central venous devices: definition of minimal requirements for training. British Journal of Anaesthesia. 110: 347 – 356
[7] Schmidt, G.A. Kory, P (2013) Ultrasound – guided central venous catheter insertion; teaching and learning. Intensive Care Medicine. Available online
[8] Troianos, C.A. Hartman, G. S. Glas, K. E (2011) Guidelines for Performing Ultrasound Guided Vascular Cannulation Recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anaesthesiologists. Journal of the American Society of Echocardiography. 24: 1291 – 1318
[9] National Institution for Clinical Excellence (NICE) (2014) Infection Prevention and Control. Nice Quality Standards – Vascular Access Devices (QS61) [Available online] https://www.nice.org.uk/guidance/qs61/chapter/quality-statement-5-vascular-access-devices. Accessed March 2016
[10] Bunting J, Slaughter R, Masel P, Kroll W, Bell S (2000) Ultrasound placement of peripherally inserted central catheters (PICCs) in adults with cystic fibrosis, Thorax 55(6): 535
[11] National Institute for Clinical Excellence (NICE). Guidance on the use of ultrasound locating devices for placing central venous catheters. Technology Appraisal Guidance No. 49. London: NICE; 2002.