Following device insertion, it is critical that the device is managed correctly to prevent post insertion complications. According to Loveday et al (2014)[1] and Moreau et al. (2013)[2] Healthcare workers caring for patients with intravascular catheters should be trained and assessed as competent in using and consistently adhering to practices for the prevention of catheter-related bloodstream infection. In this final article, we explore best practices for maintaining and removing CVCs.
Is the CVC Still Required?
The first step to CVC care and maintenance is to assess whether it is still required, or if it is causing harm to the patient by being in situ. It is important to follow your organisations Care Bundles and local guidelines, where available.
If the CVC is still required, and not causing harm to the patient in anyway, the next step is to ensure the area around the CVC is secure and a suitable barrier from bacteria and other sources of infection.
Aseptic Non-Touch Technique (ANTT®)
We discussed in the previous article the meaning and practice of Aseptic non-touch technique (ANTT®), but this mention serves as an important reminder to maintain the asepsis of procedure key parts[3] and always work with ANTT® techniques, referring to your organisations policy on these techniques for dressing and flushing vascular access devices.
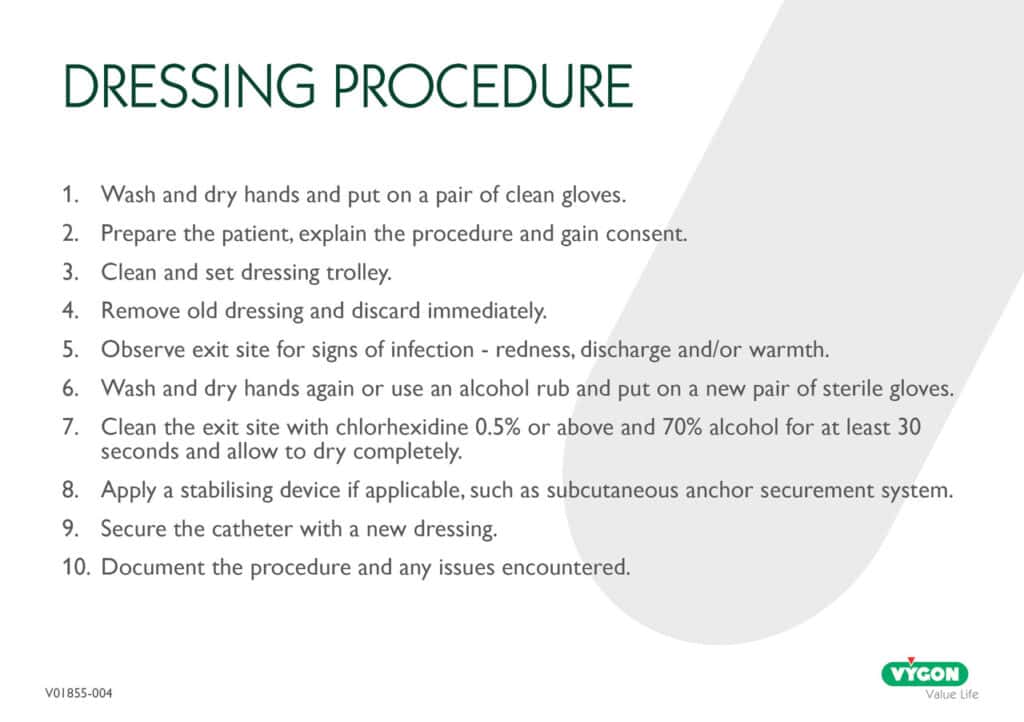
Dressing Regimens and Procedures
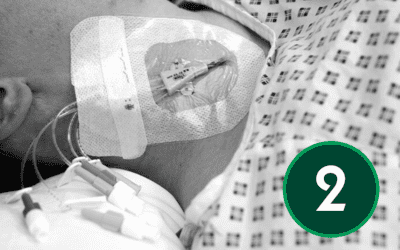
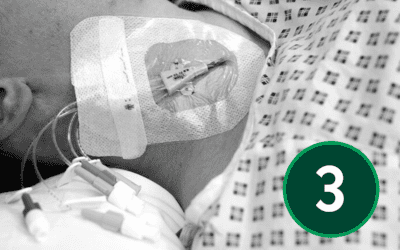
An appropriate dressing for catheter sites is one that supports secure fixation, allows easy visual monitoring of the area, and maintains a protective barrier. It should also allow the skin to breathe while shielding the site from external moisture and contaminants.
Although the following section reflects widely accepted best‑practice principles for CVC care, dressing products, change intervals, and site‑care procedures differ across organisations. Local Trust policy must always take precedence.
- Use aseptic non-touch technique when accessing the CVC.
- Dressing should be:
- Transparent to allow visual inspection of the site
- Self-adhesive to provide stability and reduce the risk of vein intima trauma, phlebitis, and contamination.
- Semi-permeable, protecting the site from bacteria and liquids while allowing the skin to breathe[4].
- Inspect dressings at each shift change to ensure integrity and cleanliness.
- Change dressings in accordance with your local Trust policy, typically dressings are changed every 7 days, 3 days, or 72 hours, or sooner if no longer intact, or if moisture collects under the dressing.
- If the patient has profuse perspiration, or the insertion site is bleeding or oozing, a sterile gauze dressing can be used. This will require daily inspection and replacement if it becomes damp, loose, or soiled3).
- Replace gauze dressings with transparent dressings as soon as possible3.
Maintaining Catheter Patency
Vascular access catheter occlusions are a common problem. However, it is important that the function of a CVC is maintained to prevent disruption in patient treatment.
Mechanical Occlusion
Occlusions can be mechanical. These types of occlusions are caused by inadequate function of some part
of the administration set-up, the dressing or the catheter that interrupts the flow. Some of these occlusions are easily identified, such as kinks or closed clamps. Others are less obvious and can be caused by the internal positioning of the CVC6. Mechanical occlusions can be ruled out by checking the following:
- IV tubing – is it clamped or kinked?
- Are all connections tight with no air leaks?
- Is the catheter kinked, twisted or misplaced?
- Does the changing of patient position improve the situation?
If these strategies do not allow the aspiration or delivery of medication the patient should be referred for further investigation of their device.
Blood Occlusion
Blood occlusions occur when a clot completely occludes the lumen of the CVC. Blood occlusions can occur suddenly or over time. Failure to correctly flush a device is a common cause of catheter occlusion.
Persistent Withdrawal Occlusion
The body reacts to any irritant in the vascular system by depositing fibrin around the irritant. In vascular access devices the body sees the catheter as a foreign object and deposits fibrin and thrombus around it[5]. The first sign of a fibrin sheath is the inability to withdraw blood from the catheter. The vacuum created by negative pressure of withdrawal pulls back a flap, which is formed by the fibrin sheath, against the catheter opening and this prevents blood from entering the lumen. Fluids however can be delivered freely.
The catheter must be aspirated to ensure blood return prior to the delivery of medications or solutions[6]. However, according to the RCN (2010), there is no requirement to routinely withdraw blood and discard it prior to flushing (except prior to blood sampling although the first sample can be used for blood cultures)[7].
CVC Clearance / Flushing
While the following flushing guidance reflects widely accepted best‑practice principles for maintaining CVC patency, specific flush volumes, solutions, and procedures vary between hospitals. Clinicians must always follow their local Trust protocols
- Flushing of CVCs is important for maintaining catheter patency1
- Catheters should be flushed with 0.9% normal saline
- Devices should be flushed prior to and following each infusion6
- A turbulent flush should be used by using a ‘push / pause’, stop / start positive pressure technique
- This will help to remove debris from the internal catheter wall
- CVC are designed to withstand venous infusion pressures but typically infusion pressures should never exceed 25-40 pounds per square inch (PSI). Therefore, syringes used for flushing of central venous access devices should be no smaller than 10mLs. Smaller syringe sizes will generate excessive pressures and could lead to catheter fraction8
- Heparin should be used as per manufacturer and local guidelines and policies
Other Considerations
Some additional considerations to ensure the longevity for the maintenance and care of a CVC include:
- The use of sutureless securement devices could be utilised[9], such as subcutaneous anchor securement systems.
- Needleless connectors should be changed as per manufacturer recommendations4
- Use a designated catheter lumen to administer lipid- containing parenteral nutrition or other lipid-based solutions
- Documentation should be maintained4
- Hands must be decontaminated, with an alcohol-based hand rub or by washing with liquid soap and
- water if soiled or potentially contaminated with blood or body fluids, before and after any contact with the intravascular catheter or insertion site1
- Use ANTT® for the insertion and care of an intravascular access device and when administering intravenous medication.1
Removing a CVC Safely
CVCs should be removed as soon as they are no longer required or if they are causing the patient harm1. They should only be removed by competent practitioners. The patient should be prepared for the removal procedure, in the same way as when preparing for inserting the CVC in article 1 and 2.
Removal Procedure
Being aware of the risks of removal is just as important as the risks of insertion, and most of these risks carry over to this procedure.
During CVC removal the middle layer of the vein, Tunica Media, is stimulated. This can lead to venospasm, which will result in difficulty in removing the catheter, making the catheter feel as if it is ‘stuck’. To reduce spasm, it is worth pausing the procedure for a short time and retrying. If it continues, it is important to contact an Interventional Radiologist for advice and assistance.
It is well documented that air embolism can occur post device removal and, therefore, it is imperative that a bioclusive dressing is applied and the patient is given instructions on how to recognise this critical complication, and what steps they should take if they suspect it.
Once the practitioner understands and mitigates all the risks, as before, they may start the removal of the CVC, to do this, they must[10],[11]:
Patient Preparation
- Check patient identity.
- Explain procedure to patient.
- Gain informed consent.
Patient Positioning
- Ensure patient comfort.
- Ensure adequate lighting and ventilation.
- The patient should be placed in the Trendelenburg position.
- This means that the exit site is below the heart and thus the risk of air embolism will be reduced.
- Instruct the patient to take a deep breath and hold it.
- Remove the CVC
Prepare Trolley
- Wash hands or if hands visibly clean use alcoholic hand rub.
- Clean and set trolley.
- Remove old dressing.
- Decontaminate hands with alcohol rub and put on clean gloves.
- Sutures or securement device should be removed and disposed of.
Clean Site
- Clean site using chlorhexidine 2% in 70% alcohol.
Removal Process
- Remove catheter – there should be no resistance.
- Firm digital pressure should be applied for at least five minutes.
- An occlusive dressing should then be applied.
Following Procedure
- Routine culture of tips is no longer considered necessary.
- Document the procedure.
Conclusion
Proper care and timely removal of central venous catheters (CVCs) are vital to preventing complications and ensuring ongoing patient safety. Regular assessment of catheter necessity, adherence to aseptic techniques, and effective flushing and dressing practices help prolong the catheter’s lifespan. When removal is required, it must be performed by competent professionals, with close attention to patient preparation and post-procedure care. By following these best practices, healthcare teams can confidently deliver safer, more effective vascular access and management, improving patient outcomes and reducing infection risks along the way.
Continue Reading
- Article 1: Understanding CVCs: Roles, Anatomy, and Device Selection

- Article 2: Preparing for CVC Insertion – Patient Assessment, Consent, and Pain Management

- Article 3: Infection Prevention and Aseptic Techniques

- Article 4: Foundations of Ultrasound Physics and Applications

- Article 5: Central Venous Lines – Insertion Techniques and Pain Management

- Article 6: Navigating Complications in Central Venous Access

- Article 7: Post-Insertion Care, Maintenance and Safe Removal

References
[1] Loveday, H.P., Wilson, J.A., Pratt, R.J., Golsorkhi, M., Tingle, A., Bak, A., Browne, J., Prieto, J. & Wilcox, M. (2014). epic3: National evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England. Journal of Hospital Infection, 86(Supplement 1), S1–S70.
[2] Moureau N, Lamperti M, Kelly LJ, et al. Evidence-based consensus on the insertion of central venous devices. Br J Anaesth. 2013;110:347–56.
[3] Rowley S, Clare S. ANTT: a standard approach to aseptic technique. Nursing Times. 2011;107(36):12‑14.
[4] National Infection Prevention and Control Manual. Central venous catheter (CVC) insertion and maintenance: Adult guidance. Health Protection Scotland; 2023.
[5] Santilli, J.S. (2002). Fibrin sheaths and central venous catheter occlusions: Diagnosis and management. Techniques in Vascular and Interventional Radiology, 5(2), 89–94.
[6] Infusion Nurses Society. Infusion Therapy Standards of Practice. 2016. (Referenced in Standard 50 and Standard 68 summarised in: “Catheter Blood Return Guidelines & Best Practices”).
7 Royal College of Nursing. Standards for infusion therapy. 3rd ed. London: Royal College of Nursing; 2010.
8 Hadaway, L (2010) Technology of flushing vascular access devices. Journal of Infusion Nursing. 29 (3) 137 – 145
9 O’Grady NP, Alexander M, Burns LA, Dellinger EP, Garland J, Heard SO, et al. Guidelines for the prevention of intravascular catheter‑related infections. Centers for Disease Control and Prevention; 2011.
10 Dougherty L. Central venous access devices: care and management. Oxford: Blackwell Publishing; 2006.
[11] Bodenham A, Babu S, Bennett J, Binks R, Fee P, Fox B, et al. Safe vascular access 2016. Anaesthesia. 2016;71(5):573‑585.