Necrotising enterocolitis (NEC) is one of the most devastating gastrointestinal emergencies in neonatal care, predominantly affecting preterm and very low‑birth‑weight infants. Its prevalence can reach 11% in VLBW infants and 22% in ELBW infants, with mortality climbing to over 50% among those requiring surgery. Survivors remain at high risk for long‑term complications such as neurodevelopmental impairment and intestinal failure. NEC’s unpredictability and rapid progression make it a crucial consideration in all enteral feeding decisions [1].
Although its exact cause remains multifactorial, prematurity continues to be the strongest predictor. Immature intestinal barriers, altered microbial colonisation, and dysregulated inflammatory pathways create a perfect storm of vulnerability.
Additional modifiable factors – including formula feeding, prolonged antibiotic exposure, slow progression to full enteral feeds, and prior blood transfusions – have all been strongly associated with increased NEC risk. Formula feeding has been repeatedly linked to higher NEC incidence due to the absence of protective immunological and microbial components found in human milk. [2,3]
In a large prospective case‑control study, infants who were formula‑fed were twice as likely to develop NEC compared with those receiving human milk, highlighting the significant impact that early nutritional choices can have on intestinal stability and microbial colonisation patterns. Prolonged antibiotic exposure has also been identified as a contributor to NEC risk by disrupting normal microbiome development and promoting dysbiosis, a known precursor to abnormal inflammatory responses seen in NEC. [5]
Delayed attainment of full enteral feeds may further exacerbate risk by prolonging the period in which the gut receives insufficient trophic stimulation, potentially impairing mucosal integrity and motility. Infants who took longer to reach full feeds were significantly more likely to develop NEC in the same case‑control study, suggesting that feed advancement protocols play an important role in shaping intestinal resilience. Among the most striking findings was the association between prior blood transfusion and NEC: affected infants demonstrated a dramatically higher risk, with transfusion exposure emerging as one of the strongest predictors in multivariate analysis. Although the mechanism remains debated, hypotheses include inflammation amplified by transfusion reactions, changes in mesenteric blood flow, or increased vulnerability during feeding around the time of transfusion. This cluster of modifiable factors serves as a reminder that while prematurity remains the dominant driver of NEC, careful attention to feeding type, antibiotic stewardship, feeding advancement, and transfusion practices can meaningfully alter risk trajectories in vulnerable infants.[5]
NEC – Recognising the Signs
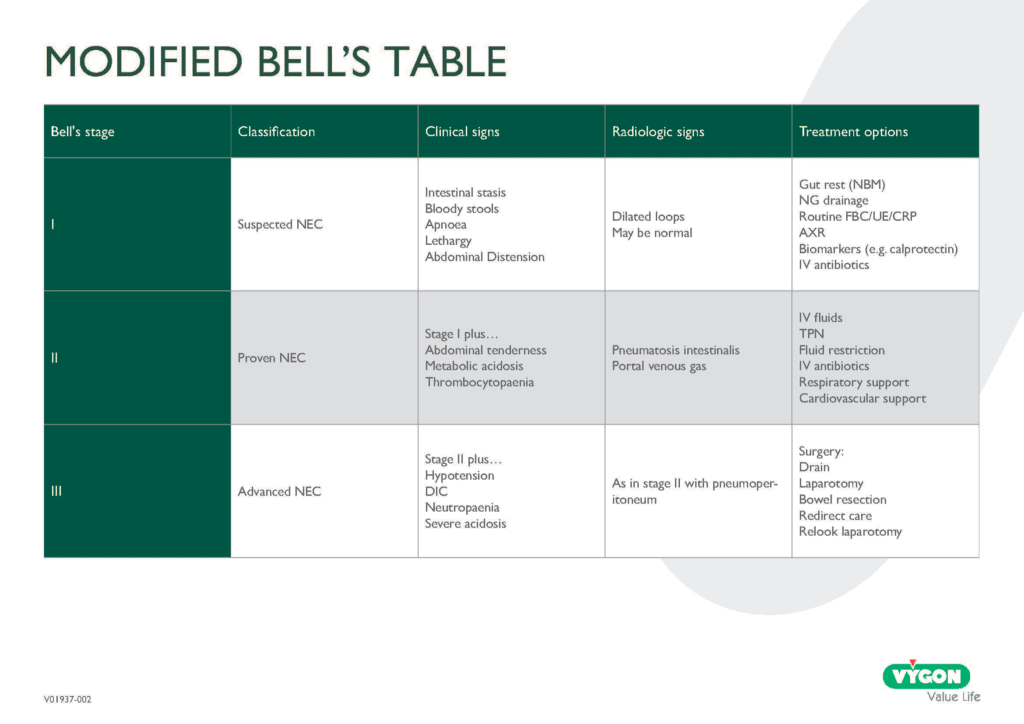
Clinical presentation is often abrupt: abdominal distension, feeding intolerance, lethargy, and bloody stools. Diagnosis relies on clinical signs paired with imaging findings such as pneumatosis intestinalis. Early recognition is critical because NEC can evolve from mild inflammation to full intestinal necrosis within hours. Evidence‑based guidelines emphasise rapid staging and management using modified Bell’s criteria to guide interventions from bowel rest and gastric decompression to surgical exploration in advanced disease. [6]
Management aims to stabilise the infant, prevent progression, and support systemic function. This includes cessation of enteral feeds, broad‑spectrum antibiotics, ventilation support if necessary, and careful fluid resuscitation. Emerging research into donor human milk, probiotics, and targeted microbial therapies offers hope for prevention, though effectiveness varies across populations and formulations. [5]
Within the context of this series, NEC is an essential link between foundational enteral nutrition principles and the next article’s focus on cleanliness and contamination control. NEC risk is directly influenced by feeding choices, microbial exposure, and device hygiene. Protecting the fragile neonatal gut requires not only biological understanding but also meticulous control of feeding systems, connectors, and milk handling practices -underscoring why cleanliness can never be optional in neonatal nutrition.
Next Article:

Cleanliness in Enteral Feeding: Protecting the Most Vulnerable
References
[1] Hu, X., Liang, H., Li, F. et al. Necrotizing enterocolitis: current understanding of the prevention and management. Pediatr Surg Int 40, 32 (2024). https://doi.org/10.1007/s00383-023-05619-3
[2] Schanler RJ, et al. Randomized trial of donor human milk versus preterm formula as substitutes for mothers’ own milk in the feeding of extremely premature infants. Pediatrics. 2005;116(2):400–406.
[3] Quigley M, McGuire W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst Rev. 2014(4):Cd002971.
[4] Quigley M, Embleton ND, McGuire W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst Rev. 2018
[5] Kamanga NHB, Thomas R, Thandrayen K and Velaphi SC (2025) Risk factors and outcomes of infants with necrotizing enterocolitis: a case-control study. Front. Pediatr. 13:1611111. doi: 10.3389/fped.2025.1611111
[6] Carroll D, (2026) Necrotizing enterocolitis: a review of current practice and current understanding of the pathophysiology. Paediatrics and Child Health, Volume 36, Issue 1, 1 – 6
A place to learn about health procedures and techniques from leading professionals.
