In Neonatal Intensive Care Units (NICUs), vascular access is not optional, it’s essential. Over 85% of NICU patients require some form of Vascular Access (VA) during their stay. Yet, the choice of device and insertion technique can dramatically affect outcomes. Repeated failed attempts, high complication rates, and vein depletion are common issues when conventional methods are used.
This is not only a clinical problem but also a problem of excessive variation between operators. Every failed attempt means more pain for the baby, more stress for the care team, and more anxiety for the parents. So how do we fix this?
Neonatal Vascular Access and the Use of the Modified Seldinger Technique
We joined the global Vygon team, with Roland Van Rens who hosted a masterclass webinar focusing on the Modified Seldinger Technique (MST).
The webinar considered the unique challenges of neonatal vascular access and the importance of choosing the right device and insertion technique. Roland explored the principles and application of MST, reviewed evidence supporting its use within Neonatology, and looked at practical implantation and training considerations.
Roland also explored Vascular Access Management Plans (VAMP), and how to avoid creating Difficult Intravenous Access Patients (DIVA), and the 7 rights of vascular access, in relation to neonatology, which created an interesting discussion piece.
If you missed it, and want to learn more about Vascular Access in Neonatology, you can still register to access the recording on Campus Vygon.
The importance of choosing the right device & insertion technique
During the webinar, Roland van Rens presented compelling data from a large-scale retrospective cohort study conducted in a NICU in Doha, Qatar. The study spanned three years and analysed 1,445 catheter insertions, comparing conventional techniques with MST using a dedicated micro-insertion kit.
Key Findings from the Study
- First-Attempt Success Rate
- Conventional technique: 88%
- MST: 91%
This improvement, though seemingly modest, is clinically significant. In neonatal care, every additional attempt increases the risk of trauma, infection, and stress for the baby. A higher first-attempt success rate means fewer punctures, less pain, and faster access to therapy.
- Complication Reduction
- Conventional technique: 39 complications
- MST: 8 complications
The types of complications tracked included catheter damage, accidental removal, occlusions, leakage, infections, extravasation, and infiltration. MST’s design using a micro-puncture needle and soft guidewire minimises vessel trauma and reduces the likelihood of these adverse events.
- CLABSI Rate (Central Line-Associated Bloodstream Infections)
- Conventional technique: 3.45 per 1,000 catheter days
- MST: 1.06 per 1,000 catheter days
This represents a 69% reduction in bloodstream infections, a critical metric in neonatal care. Lower CLABSI rates translate to improved patient outcomes, shorter hospital stays and reduced antibiotic use.
- Catheter Longevity
MST also contributed to longer catheter dwell times. With fewer complications and better insertion success, catheters remained functional for extended periods, reducing the need for repeated procedures and preserving venous access.
From Technique to Strategy: VAMP
Implementing MST is not just about switching tools, it’s about changing mindset. The webinar introduced the concept of a Vascular Access Management Plan (VAMP), built on the “7 Rights of Neonatal Vascular Access”:
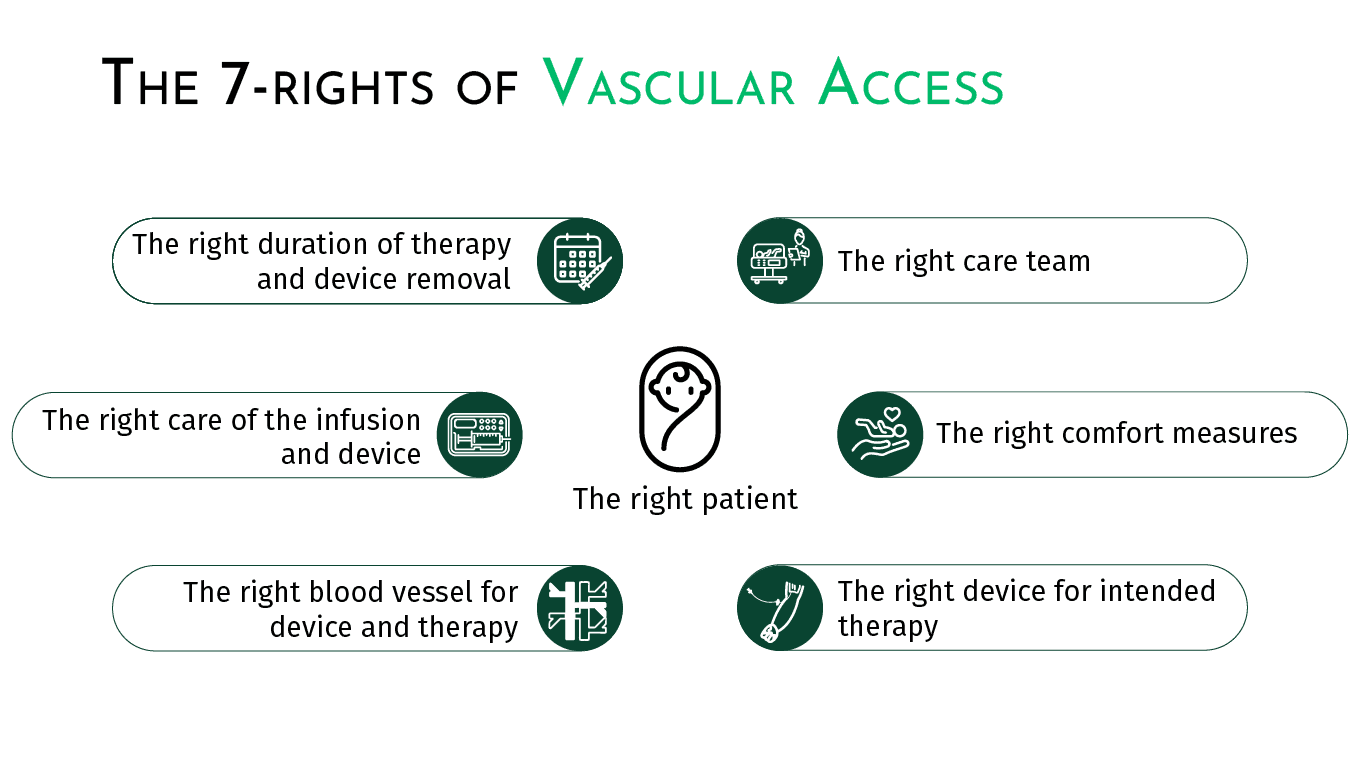
This proactive approach replaces reactive decisions made only when a catheter fails. With a global approach and a structured VAMP, teams can anticipate access needs, reduce complications, and improve the overall experience for patients, families, and healthcare professionals.
Training and Teamwork: The Key to Success
MST requires proper training. It’s not enough to have the right kit. You need the right skills. The webinar emphasised the importance of:
- Standardised training programs
- Hands-on training simulation
- Visualisation of veins using ultrasound
A dedicated vascular access team including nurses, neonatologists, educators, and even parents can facilitate training, monitor outcomes, and drive continuous improvement.
Another study showed that introducing a specialised n-PICC team increased first-attempt success rates from 58.6% to 67.2%, and overall success from 81.7% to 97.6%. Therapy failure rates dropped from 7.4% to 4.8%.
What You Can Do Today
If you work in neonatal care, here’s how you can start making a difference:
- Evaluate your current practice: How many attempts does it take to insert a catheter? What complications are you seeing?
- Train your team: Organise MST workshops and simulations.
- Implement MST: Use neonatal-specific kits and follow the step-by-step protocol.
- Design a VAMP for each patient: Plan ahead instead of reacting to failures.
- Share your results: Track your data and celebrate improvements.
MST is more than a technique, it’s a movement toward safer, smarter, and more compassionate neonatal care.
Further Global Validation
The webinar also referenced multiple international studies that support MST’s effectiveness:
- Song et al. (2018): Randomised controlled trial showing MST increased success rates from 65% to 83%.
- Gupta et al. (2021): Retrospective study with 100 catheters showing fewer punctures per successful insertion.
- Gibb et al. (2021): Retrospective study with 57 catheters showing an increase of first attempt, fewer punctures per successful insertion and cost effectiveness.
- Rodriguez et al. (2023): RCT showing clinical benefits, though not statistically significant.
- Zinni et al. (2024): Prospective study reporting 100% success with no complications.
- Van Rens et al. (2024): The Qatar study cited above, with the largest cohort and most comprehensive outcome analysis.
These studies collectively demonstrate that MST is not only effective in controlled environments but also adaptable across diverse clinical settings.
References
Legemaat M, Carr PJ, van Rens RM, van Dijk M, Poslawsky IE, van den Hoogen A. Peripheral intravenous cannulation: complication rates in the neonatal population: a multicenter observational study. J Vasc Access. (2016) 17(4):360–5. doi: 10.5301/jva.50005582025-10
Odom B, Lowe L, Yates C. Peripheral infiltration and extravasation injury methodology: a retrospective study. J Infus Nurs. (2018) 41(4):247–52. doi: 10.1097/NAN.00000000000002872025-10
Van Rens MFPT, Hugill K, Mahmah MA, et al. Evaluation of unmodifiable and potentially modifiable factors affecting peripheral intravenous device-related complications in neonates: a retrospective observational study. BMJ Open. (2021) 11(9):e047788. doi: 10.1136/bmjopen-2020-0477882025-10
Bayoumi MAA, van Rens MFPT, Chandra P, et al. Effect of implementing an Epicutaneo-Caval Catheter team in Neonatal Intensive Care Unit. J Vasc Access. (2021) 22(2):243–253. doi: 10.1177/11297298209281822025-10
Van Rens MFPT, Hugill K, van der Lee R, et al. Comparing conventional and modified Seldinger techniques using a micro-insertion kit for PICC placement in neonates: a retrospective cohort study. Front Pediatr. (2024) 12:1395395. doi: 10.3389/fped.2024.13953952025-10
Van Rens M, Ostroff M, Bayoumi MAA. The Modern Role of Neonatal PICCs Subspecialty. Nurs Crit Care. (2025) 30(4):e70111. doi: 10.1111/nicc.701112025-10
McIntyre C, August D, Cobbald L, et al. Neonatal Vascular Access Practice and Complications: An Observational Study of 1,375 Catheter Days. J Perinat Neonatal Nurs. (2023) 37(4):332–339. doi: 10.1097/JPN.00000000000005892025-10
D. August et al. Peripheral intravenous catheter practices in Australian and New Zealand neonatal units: A cross-sectional survey. Journal of Neonatal nursing. doi.org/10.1016/j.jnn.2019.03.002. (2019 October)
Van Rens MFPT, Bayoumi MAA, van de Hoogen A, et al. The ABBA project (Assess Better Before Access): A retrospective cohort study of neonatal intravascular device outcomes. Front Pediatr. 2022;10:980725. (Published 2022 Nov 3). doi:10.3389/fped.2022.980725