Midline catheters are designed to provide stable, medium‑term intravenous therapy, typically when treatment is expected to exceed the limits of short peripheral cannulas (3-4 days), where the treatment does not require central venous access. Accurate device selection is increasingly recognised as essential for preserving vessel health, preventing avoidable complications, and improving patient experience. Published guidelines emphasise the importance of choosing the right vascular access device early, with a structured approach to assessment, ultrasound‑guided placement, and adherence to vessel health and preservation principles to minimise harm[1].
Recent evidence underscores the safety advantages of midlines in appropriate clinical scenarios. Several systematic reviews and cohort studies have shown that midline catheters are associated with lower rates of catheter‑related bloodstream infections (CRBSIs) compared with peripherally inserted central catheters (PICCs), making them a valuable alternative when central access is not clinically required[2],[3],[4]. This reduction in infection risk has contributed to the increasing adoption of midlines in settings seeking to minimise central line exposure
By framing midline selection within evidence‑based practice, clinicians can optimise safety, reduce complications, and ensure patients receive the most appropriate device for their therapy needs.
When a Midline Should Be Considered
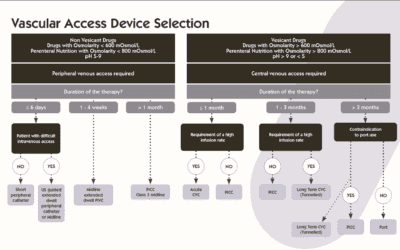
Midlines are most suitable when intravenous therapy is expected to last more than six days, provided the medication is non‑vesicant, non‑irritant, and within a pH range of 5-9[5]. This makes them a strong option when a peripheral cannula is no longer appropriate and central access is not clinically required.
When selecting a vascular access device, INS guidance recommends considering anticipated duration of therapy, medication properties (pH, osmolarity, vesicant/irritant status), the patient’s vascular history and comorbidities, and risk of complications, such as thrombosis, infection, extravasation.[6]
However, midline use may increase infiltration and extravasation risk, and recommendations are that midlines should not be used for vesicants, parenteral nutrition, or solutions with extreme pH or osmolarity due to insufficient evidence[7].
Why Choose a Midline Over Other Vascular Access Devices?
Midlines vs Peripheral Cannulas
Midlines demonstrate lower bloodstream infection rates than PICCs in multiple studies, though superficial thrombosis risk may be higher. They are not a universal substitute for PICCs, particularly when central access is clinically indicated.⁵
Midlines vs PICCs
Midlines demonstrate several important differences in performance when compared with PICCs. Systematic reviews and multicentre studies show that midlines are associated with lower bloodstream infection rates than PICCs, highlighting a clear safety advantage in suitable patients.2,3,4
However, while overall thrombosis risk does not differ, midlines are linked with higher rates of superficial venous thrombosis, indicating the need for careful monitoring.2
Evidence also shows that midlines may experience higher total complication rates in some settings, including leakage or premature removal, which reinforces the need for appropriate device selection based on therapy, duration, and patient factors.3
Randomised and controlled evidence further clarifies that midlines should not be used as blanket replacements for PICCs.
In particular, patients who have been referred for PICC placement may not experience equivalent outcomes when switched to midlines, underscoring the importance of individualised assessment rather than universal substitution.4
Overall, the evidence supports a nuanced approach: midlines are highly effective when used appropriately but should be chosen selectively rather than as universal PICC alternatives.
Midlines vs Central Venous Catheters
Midlines have been shown to offer lower complication rates, including reduced thrombosis, catheter‑related infections, and catheter blockage, when compared with central venous catheters, provided the therapy is appropriate for peripheral delivery. They also demonstrate longer mean dwell times than CVCs in available evidence, supporting their use as a safer and more durable option in suitable patients.3
| Category | Midlines | PICCs | CVCs |
| Bloodstream infection (CRBSI) | Lower CRBSI rates than PICCs2,3,,4. | Higher CRBSI risk vs midlines2. | Higher CRBSI risk compared with midlines3. |
| Thrombosis | Similar DVT/PE risk but higher superficial thrombosis2. | Similar DVT/PE risk; lower superficial thrombosis2. | Higher thrombosis risk overall3. |
| Total complication rates | Higher complication rates in some settings2,3. | Lower total complication rates3. | Higher complication risk due to invasiveness3. |
| Dwell time | Longer mean dwell vs CVCs3. | Longer dwell than midlines3. | Shorter dwell; for high-acuity use. |
| Invasiveness | Peripheral device; lower risk. | Central device; more complex. | Most invasive; highest risk. |
| When preferred | Medium-term therapy (>6 days), peripheral-compatible drugs. | When central access required or therapy unsuitable for midlines. | Critical care, rapid infusions, central therapies. |
The Role of Specialist Vascular Access / Vascular Management Teams
Safe and effective vascular access depends on trained professionals, and current guidelines highlight the importance of dedicated vascular access teams, the consistent use of ultrasound, and correct catheter‑to‑vein ratios within broader vessel health strategies.1 These teams reduce complication risks by ensuring evidence‑based practice and maintaining high procedural standards.
Specialist involvement is particularly valuable when advanced techniques are required, or the patient has difficult intravenous access (DIVA). PICC studies show that tunnelling and tip‑related technologies can significantly reduce complications such as infection, thrombosis, and dislodgement, reinforcing the benefit of skilled operators for complex access needs[8],[9].
For midlines, this supports recommending specialist team input for assessment and placement, especially when stability, longevity, or patient‑specific challenges must be considered.
Technique Considerations: Tunnelling
Tunnelling refers to creating a short subcutaneous tract between the vein entry site and the skin exit site, and its purpose is to stabilise the catheter, reduce infection risk, and support longer dwell times.
Although dedicated midline tunnelling studies remain limited, evidence from peripherally inserted central catheter practice indicates that tunnelling may help reduce complications such as infection, thrombosis, and dislodgement, and ongoing multicentre trials are expected to provide further validation of these benefits[10].
Consequently, tunnelling is a technique with emerging evidence and growing interest for improving line integrity and longevity.
Key Clinical and Practical Considerations
Medication compatibility
Medication compatibility is a critical consideration when selecting a vascular access device, including a midline, as these devices are not suitable for vesicant drugs, solutions with extreme pH or osmolality, or continuous parenteral nutrition infusion. These therapies carry a significantly higher risk of extravasation injury, and current evidence remains insufficient to safely support midline administration of such fluids.7 Clinicians should therefore assess the biochemical properties of prescribed medications before choosing a midline to avoid preventable complications.
Ultrasound‑guided insertion
Ultrasound‑guided insertion should be regarded as standard practice for midline placement, as supported by current vascular access guidelines.1 Real‑time ultrasound enables accurate vessel identification, optimises vein selection, and reduces insertion‑related complications such as arterial puncture or failed cannulation. Consistent use of ultrasound guidance contributes to improved procedural success rates and safer overall care.
Clinical and therapy considerations
Appropriate midline use also depends on practical considerations such as therapy duration, the patient’s mobility, securement needs, dressing selection, and regular assessment of device necessity. These factors influence both dwell time and complication risk, making regular multidisciplinary review essential. Care teams should evaluate whether the prescribed treatment still requires a midline or whether an alternative device would offer better vessel preservation and safety[11].
Vessel health and preservation
Vessel health and preservation principles must underpin all decisions regarding midline insertion. This includes conducting early vascular access assessment, selecting the most appropriate device on the first attempt, and with ongoing reassessment of the line throughout therapy.[12] Applying these principles supports long‑term vessel integrity, reduces device‑related complications, and promotes high‑quality vascular access practice.
Conclusion
Midlines are a safe and effective vascular access option when used for the right therapies and durations, and current evidence demonstrates their value in reducing bloodstream infections, improving patient comfort, and preserving vessels when compared with repeated cannulation or unnecessary central access. Achieving the best possible outcomes depends on matching the correct therapy and patient type, getting involvement from specialist vascular access teams, the use of appropriate insertion techniques including the growing interest in tunnelling, and consistent adherence to evidence-based guidelines.
References
[1] Johnston AJ, Simpson MJ, McCormack V, Barton A, Bennett J, Chalisey A, et al. Association of Anaesthetists guidelines: safe vascular access 2025. Anaesthesia. 2025 Sep 17;80(11):1381–96. doi:10.1111/anae.16727.
[2] Urtecho M, Torres Roldan VD, Nayfeh T, et al. Comparing Complication Rates of Midline Catheter vs Peripherally Inserted Central Catheter: A Systematic Review and Meta‑analysis. Open Forum Infect Dis. 2023.
[3] Canadian Agency for Drugs and Technologies in Health (CADTH). Midline catheters for administering intravenous infusion therapy. 2025. Available from: https://www.cda-amc.ca/sites/default/files/pdf/htis/2025/RC1572_Safety_of_Midline_Catheters.pdf
[4] Swaminathan L, Flanders S, Horowitz J, et al. Safety and Outcomes of Midline Catheters vs PICCs for Short‑Term Indications: A Multicentre Study. JAMA Intern Med. 2021.
[5] Derouin Y, Le Thuaut A, Dauvergne J, et al. Midline catheter follow‑up in non‑ICU patients: midDATA study protocol. BMJ Open. 2023.
[6] Optimus Vascular. INS‑Based Guide to IV Access Device Selection. 2026
[7] Hadaway L, Gorski LA. Infiltration and Extravasation Risk with Midline Catheters: A Narrative Review. 2024.
[8] Hong J, Mao X. Complications of tunneled and non-tunneled peripherally inserted central catheter placement in chemotherapy-treated cancer patients: a meta-analysis. Front Surg. 2024;11:1469847. Available from: https://www.frontiersin.org/journals/surgery/articles/10.3389/fsurg.2024.1469847/full
[9] Ceratti RN, Taxbro K, Chopra V, et al. Tunneled peripherally inserted central catheter versus non-tunneled and its effects in clinical outcomes: a multicenter randomized clinical trial protocol. PLOS One. 2026 Mar 10. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0342385
[10] Chopra V, et al. Tunnelling to prevent complications in vascular access devices. PLoS One [Internet]. Available from: https://journals.plos.org
[11] NHS Ayrshire & Arran. Midline catheter insertion (G123) guideline. 2025. Available from: https://www.rightdecisions.scot.nhs.uk/nhs-ayrshire-arran-guidelines/clinical-guidelines/preopanaesthesiabloods/midline-catheter-insertion-g123/
[12] Infection Prevention Society (IPS). Vessel Health and Preservation Framework. 2023. Available from: https://www.ips.uk.net/about-us/vessel-health-and-preservation-framework/