
In Intravenous Therapy Teams, PICC placement using standard MST (Modified Seldinger Technique) is common practice and generally well controlled. However, complications can arise if the standard technique is applied, and the insertion site is unsuitable. Failure to consider the best possible location from the inside (best vein) and the outside (best location on the arm) leads to risks that compromise the vascular access device. In these cases, two main approaches are required: the ZIM method and tunnelling.
THE ZIM METHOD: IMPORTANCE OF THE INSERTION SITE
The performance of a Vascular Access Device (VAD) can be predicted based on four criteria:
• Tip position
• Insertion technique
• Cannulated vein
• Exit site
In general, the puncture site to reach the vein is the same point as the catheter exit site. However, the ideal vein for inserting the device must meet a set of criteria (calibre, route, location on the arm) to ensure that the catheter can be maintained in good condition. We know that failure to meet these criteria directly affects the risk of thrombosis.
This is where ultrasound is key: it makes it possible to choose the best venous section with the largest possible calibre and possibly with a linear path, as well as a safe location in terms of nerve bundles and arteries.
Meanwhile, other complications, such as the incidence of infections, thrombophlebitis, and mechanical complications, depend mainly on the exit site.
In 2011, concerned about the rate of thrombosis associated with PICCs in the 2000s, vascular access expert Robert Dawson proposed a new method:
The ZIM method is a microsystem of clinical procedures designed to use ultrasound to consider the anatomy and physiology of the upper arm and reduce the risks associated with PICC insertion and use.
What is the ZIM method?
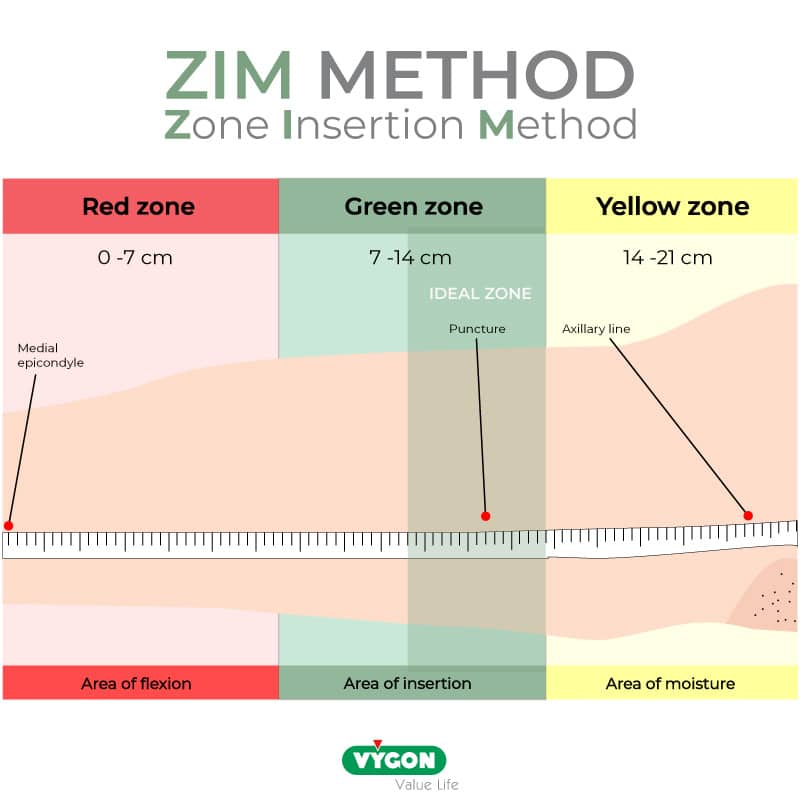
The ZIM method is the Zone Insertion Method: the arm is measured from the elbow to the axillary line—the distance is usually 20-22 cm (with a range of 18-24 cm) —and divided into three zones:
• The upper third: yellow area near the axillary area
• The middle third: green area
• The lower third: red zone near the flexure of the arm
INSERTION IN EACH ZONE OF THE ZIM METHOD
- Red zone
This portion is not recommended for venipuncture or the catheter exit site. The veins are small in calibre, and the movements of the muscles make the exit site quite unstable. This red area is related to clear complications at the time of insertion (e.g., cannulation failure, ecchymosis, etc.) and should be avoided.
- Yellow zone
This is the most proximal part and has a great advantage: the brachial section of the axillary vein is located in this area, which has a significant diameter that can reach 6-8 mm. In accordance with the rule, “the catheter must occupy a maximum of one-third of the lumen of the vein”, it enables the insertion of 6Fr catheters or even more.
The downside is that due to being located very close to the armpit, a catheter inserted in this area will present serious risks of complications. It is difficult to keep a fixation and dressing intact in this area due to sweating, thinner skin, and extensive movements due to its position in the shoulder area.
- Green Zone
This is the ideal part for venipuncture, in particular the proximal half, which is 3-4 cm wide: in this location, the brachial vein is wide in diameter and far enough away from the median nerve and arteries. Other advantages are that it is located below the muscle fasciae. Therefore, the exit site is stable, and the skin area remains dry.
However, as mentioned above, on certain occasions, it is not possible to puncture in the green zone, and/or puncturing in the yellow zone is more advantageous for the patient.
In these cases, it is essential to be able to resort to tunnelling.
WHAT IS TUNNELLING?
Tunnelling involves creating a subcutaneous tunnel from the ideal point of entry into the vein to the green zone of the ZIM method.
It is especially recommended for patients whose venous capital in the green zone is depleted or patients whose veins have a very small diameter that does not enable cannulation of the catheter with the desired calibre (remember here that a 3 mm vein is required to place a 3Fr catheter).
Tunnelling technique
Tunnelling a PICC is performed in the same way as during Hickman or port placement: the catheter is passed under the skin with a tunneller, or it can also be done with a short catheter (14G) or a long peelable cannula.
As far as the steps are concerned, there are two methods:
- Antegrade tunnelling, with a standard PICC, i.e., distal cut (tip cut):
1. The vein is cannulated to leave the guide inside
2. The tunnel is created
3. The catheter is inserted from the end point, i.e., what will be the exit point of the catheter
4. The catheter is passed into the tunnel
5. It is inserted into the vein with the MST introducer
- Retrograde tunnelling, with a PICC, using a proximal cut:
1. The vein is cannulated, and the catheter is inserted
2. The tunnel is created
3. Proximal catheter cut
4. The catheter is passed through the tunnel from the point of insertion to the point of exit
5. The final extension is assembled
Additional benefits of tunnelling
Tunnelling is a very useful resource to ensure optimal placement and avoid possible complications. In addition, it has two notable benefits:
1. It reduces infections because:
– It moves the skin entry area away from the vein entry, which reduces the risk of bacterial contamination (the subcutaneous section acts as a barrier)
– The exit tip of the catheter is in an area favourable to good catheter maintenance (away from the axillary area)
2. It reduces the risk of movement or accidental removal:
The subcutaneous part allows for better fixation of the catheter, a feature that is especially important in long-term treatment such as parenteral nutrition or chemotherapy.
Taking into account all the tools available today in the world of vascular access, such as ultrasound, the Micro Seldinger technique, the ZIM method and tunnelling, it is worth highlighting the conclusion reached by Pittiruti and Scoppettuolo in the manual GAVeCeLT:
We, therefore, have an ethical responsibility to use these tools in the best possible way, always bearing in mind that each patient has the right to maximum comfort and safety. To ignore these resources, when available, would be to risk vascular access failure together with the potential impacts on the patient’s intravenous therapy and life, both physically and emotionally.
Bibliography:
- Robert Dawson PICC Zone Insertion MethodTM (ZIMTM): A Systematic Approach to Determine the Ideal Insertion Site for PICCs in the Upper Arm, JAVA Vol 16 No 3 – 2011
- Manual GAVeCeLT sobre PICC y midline, Pittiruti y Scoppettuolo – 2016
A place to learn about health procedures and techniques from leading professionals.




