What is the challenge of performing spinal anesthesia when anatomical landmarks are impalpable?
Spinal anesthesia traditionally relies on palpable surface landmarks to guide needle insertion. In obese patients (BMI > 35) or patients with spinal deformities (scoliosis, kyphosis, prior spinal surgery), these landmarks often become unreliable, increasing technical difficulty, prolonging the procedure, and raising the probability of multiple puncture attempts which can lead to complication such as post‑dural puncture headaches.
For instance, data from the United Kingdom show that about 15% of spinal anesthetics are technically challenging, 10% require more than five attempts, and failure of central neuraxial block (CNB; spinal and epidural) may occur in roughly 5% of patients under 50 years of age. (1)
How do multiple puncture attempts increase the risk of complications in spinal anesthesia?
Multiple puncture attempts mechanically increase tissue trauma, raise the likelihood of dural puncture, and significantly elevate the risk of post dural puncture headache (PDPH). Patients with difficult anatomy (obesity, scoliosis, or prior surgery) have markedly higher first attempt failure rates, making complication prevention essential.
Key mechanisms linking repeated attempts with complications
- Higher PDPH risk: PDPH incidence rises with each additional puncture. (2)
- Soft‑tissue injury: Repeated needle attempts may cause damage to the soft tissue structures along the path of needle insertion. (1)
- Radicular pain or paresthesia: Needle misdirection can irritate nerve roots, producing transient symptoms.
- Greater procedural pain: Repeated needle redirection correlates with increased perioperative discomfort.
- Higher likelihood of block failure: Distorted trajectories reduce chances of intrathecal placement.
- Delays in care: Failed attempts prevent successful anesthetic injection, prolonging anesthesia induction and delaying the start of surgery.
The occurrence of complications is influenced by needle type, gauge, patient characteristics (age, anatomy), and operator experience.
How does difficult anatomy contribute to first‑attempt failure?
Obesity, scoliosis, kyphosis, and post‑surgical alterations distort expected surface landmarks, increasing the probability of missed midline and incorrect depth estimation. These factors multiply first‑attempt failure rates compared with normal anatomy. (1) (5)
What is pre‑procedural ultrasound and how does it help?
Pre‑procedural ultrasound (PPU) is a brief ultrasound assessment performed before inserting the spinal needle. It is used to identify the optimal intervertebral space, measure the exact depth to the intrathecal space, and determine the most appropriate needle trajectory. Unlike real‑time ultrasound guidance, PPU requires only anatomical identification and skin marking, making it easier to implement while offering substantial reductions in failed or repeated attempts.
What Pre‑procedural ultrasound (PPU) provides:
- Accurate vertebral level selection, which often differs from estimates based solely on palpation.
- Precise depth measurement from skin to intrathecal space to improve needle choice and trajectory.
- Trajectory guidance, helping decide between a midline or paramedian approach based on anatomical feasibility.
- Skin marking, enabling a single, targeted insertion point that reduces redirections and tissue trauma.
Quantified benefit
Evidence from 22 studies shows that ultrasound-assisted techniques consistently rank higher in first-pass success compared with the traditional landmark approach. Ultrasound-assisted methods show a substantially higher ranking (SUCRA 67.1%), while the landmark method ranks lowest (0.1%). SUCRA (Surface Under the Cumulative Ranking Curve) is a probabilistic measure derived from network meta-analysis, ranging from 0 to 100%, which reflects the likelihood of a technique being among the most effective, rather than its absolute clinical success rate. (1)
Evidence in obese patients: how much does ultrasound improve outcomes?
Ultrasound guidance significantly reduces the number of puncture attempts, lowers procedural pain, and improves first‑pass success in obese patients. The comparative study below shows consistent superiority of ultrasound across nearly all metrics. (4)
Comparison of Landmark vs. Ultrasound Guidance in Obese Patients
| Outcome | Landmark | Ultrasound Guindance | p value | Finding |
| Lumbar puncture time (min) | 18.43 ± 1.06 | 7.53 ± 0.95* | 0.000 | Ultrasound dramatically shortens procedure time |
| Puncture attempts (n) | 2.67 ± 1.49 | 1.13 ± 0.35* | 0.000 | Fewer attempts with ultrasound |
| First attempt success (n) | 15/30 | 26/30* | 0.005 | First attempt success nearly doubles |
| Total first attempt success rate (n) | 27/30 | 30/30 | 0.237 | not significant (p ≥ 0.05) |
| Bloody cerebrospinal fluid (n) | 9/30 | 2/30* | 0.042 | Less traumatic puncture |
| Intraprocedural sciatic nerve irritation (n) | 5/30 | 1/30 | 0.195 | not significant (p ≥ 0.05 |
| Post‑procedural low‑back pain (n) | 8/30 | 1/30* | 0.026 | Clear reduction in post‑procedure pain |
| Post‑procedural (n) | 2/30 | 0/30 | 0.492 | not significant (p ≥ 0.05 |
* Statistically significant difference compared with Group A (p < 0.05).
In obese patients, ultrasound guidance reduces puncture attempts by more than half, cuts procedure time by over 50%, and doubles the first attempt success rate while lowering pain and traumatic puncture markers.
Is ultrasound beneficial in spinal deformities?
Yes. In severe scoliosis or achondroplastic dwarfism, where palpation landmarks are absent, ultrasound greatly facilitates correct needle placement, particularly using the transverse plane. (5)
When ultrasound is particularly useful:
- Rotational deformity
- Congenital abnormalities
- Post‑laminectomy anatomy
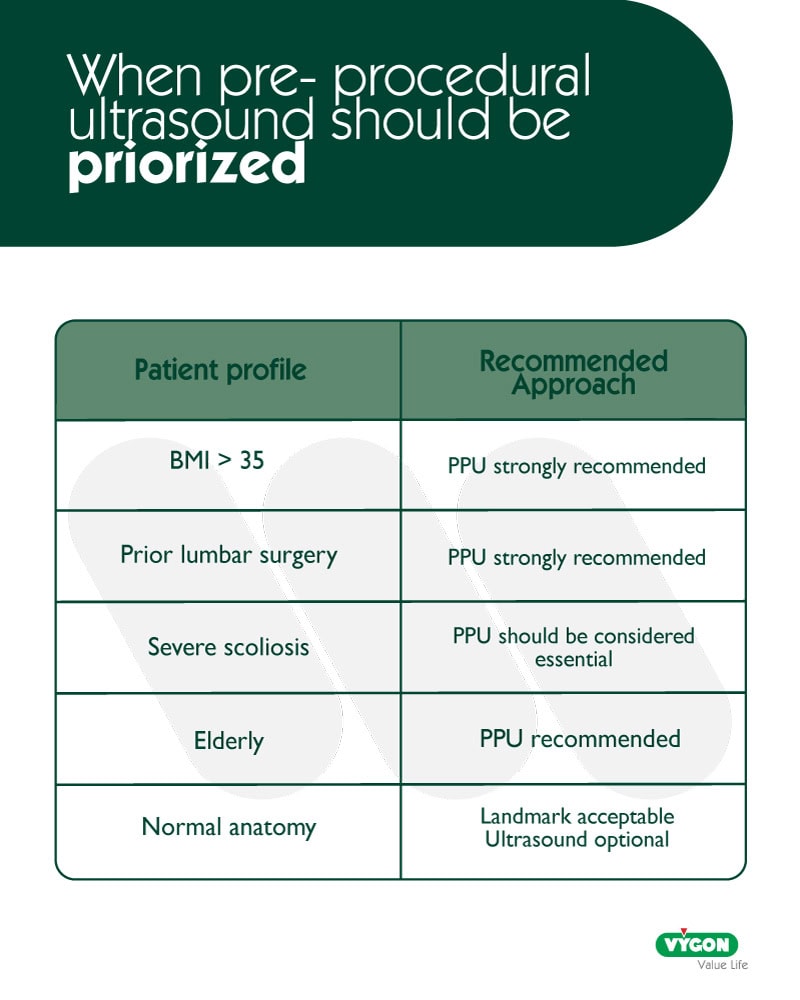
When should clinicians use pre‑procedural ultrasound?
PPU is most relevant when anatomical difficulty is expected.
- Body Mass Index (BMI) > 35
- Prior lumbar surgery
- Scoliosis or kyphosis
- Previous landmark‑based failure
- Elderly patients
Patient and organizational benefits: how much does ultrasound improve satisfaction?
Ultrasound guidance not only reduces complications and procedural pain, but also significantly increases overall patient satisfaction, as demonstrated by the comparison of satisfaction scores between landmark and ultrasound‑guided groups. (4)
Comparison of patient satisfaction (Landmark vs. Ultrasound)
| Group | n | Very satisfied | Satisfied | Dissatisfied | Total satisfaction (%) |
| Landmark | 30 | 11 | 7 | 12 | 60% |
| Ultrasound | 30 | 20 | 6 | 4 | 86.7%* |
* Statistically significant improvement compared with Group A (p < 0.05).
Ultrasound guidance increases total patient satisfaction from 60% to 86.7%, driven by fewer puncture attempts, less procedural pain, and lower complication rates.
Decision support: When ultrasound is high recommended:
Conclusion
Pre‑procedural ultrasound addresses the core challenge of spinal anesthesia when anatomical landmarks are unreliable, offering a clearer understanding of spinal anatomy before needle insertion. The evidence shows that multiple puncture attempts increase the likelihood of complications and patient discomfort, highlighting the importance of improving first‑attempt accuracy. Difficult anatomies are major contributors to technical failure, and in these cases ultrasound provides essential anatomical clarification. By identifying the correct intervertebral space, estimating depth, and defining the appropriate trajectory, ultrasound reduces first attempt and the risks associated with them. Studies in obese patients and those with spinal deformities demonstrate that ultrasound improves procedural success and patient experience. While the landmark technique remains appropriate for patients with normal anatomy, ultrasound serves as a valuable safety tool in complex situations. Overall, the conclusions across all sections support integrating pre‑procedural ultrasound into clinical practice to enhance safety, efficiency, and patient satisfaction in spinal anesthesia.
Bibliography
1. NYSORA
NYSORA. (n.d.). Ultrasound‑guided central neuraxial blocks: The evidence. Retrieved from
https://www.nysora.com/pain-management/ultrasound-guided-central-neuraxial-blocks/#toc_14–THE-EVIDENCE
2. Al‑Hashel, Rady, Massoud & Ismail (2022)
Al-Hashel, J., Rady, A., Massoud, F., & Ismail, I. I. (2022). Post-dural puncture headache: A prospective study on incidence, risk factors, and clinical characterization of 285 consecutive procedures. BMC Neurology, 22(1), 261. https://doi.org/10.1186/s12883-022-02785-0
3. Zhang, Peng, Wei et al. (Systematic Review / Network Meta‑analysis)
Zhang, Y., Peng, M., Wei, J., et al. (Year not provided). Comparison of ultrasound‑guided and traditional localisation in intraspinal anesthesia: A systematic review and network meta‑analysis. BMJ Open.
4. Li, Tao & Cai (2022)
Li, L., Tao, W., & Cai, X. (2022). Ultrasound-guided vs. landmark-guided lumbar puncture for obese patients in the emergency department. Frontiers in Surgery, 9, 874143. https://doi.org/10.3389/fsurg.2022.8741435. Kilicaslan (2023)
Kilicaslan, B. (2023). Ultrasound-guided spinal anaesthesia in a patient with achondroplastic dwarfism and scoliosis: A case report. Hong Kong Medical Journal, 29, 459–461.




