A testimonial of Dr Eric Desruennes
There aren’t many differences between children over 2 years and adults. On the other hand, newborns, infants, and children under 2 years are quite different due to:
– Their small weight and vessels, and sometimes the inappropriate size of devices
– Their short neck and elastic skin, the latter being often difficult to penetrate
– Thickness of their subcutaneous tissue
– More difficult brachial approaches for PICC-line and midline placement
As for adults, recommendations from learned societies have made the use of ultrasound mandatory, with one preferred approach in pediatrics: access through the brachiocephalic veins via a supraclavicular ultrasound-guided approach.
In this article, we will offer recommendations concerning the different steps around the placement of central venous access in pediatrics in order to ensure safe patient-centered practices that take into account the specificities and vulnerabilities of this group.
-
Central venous device choice
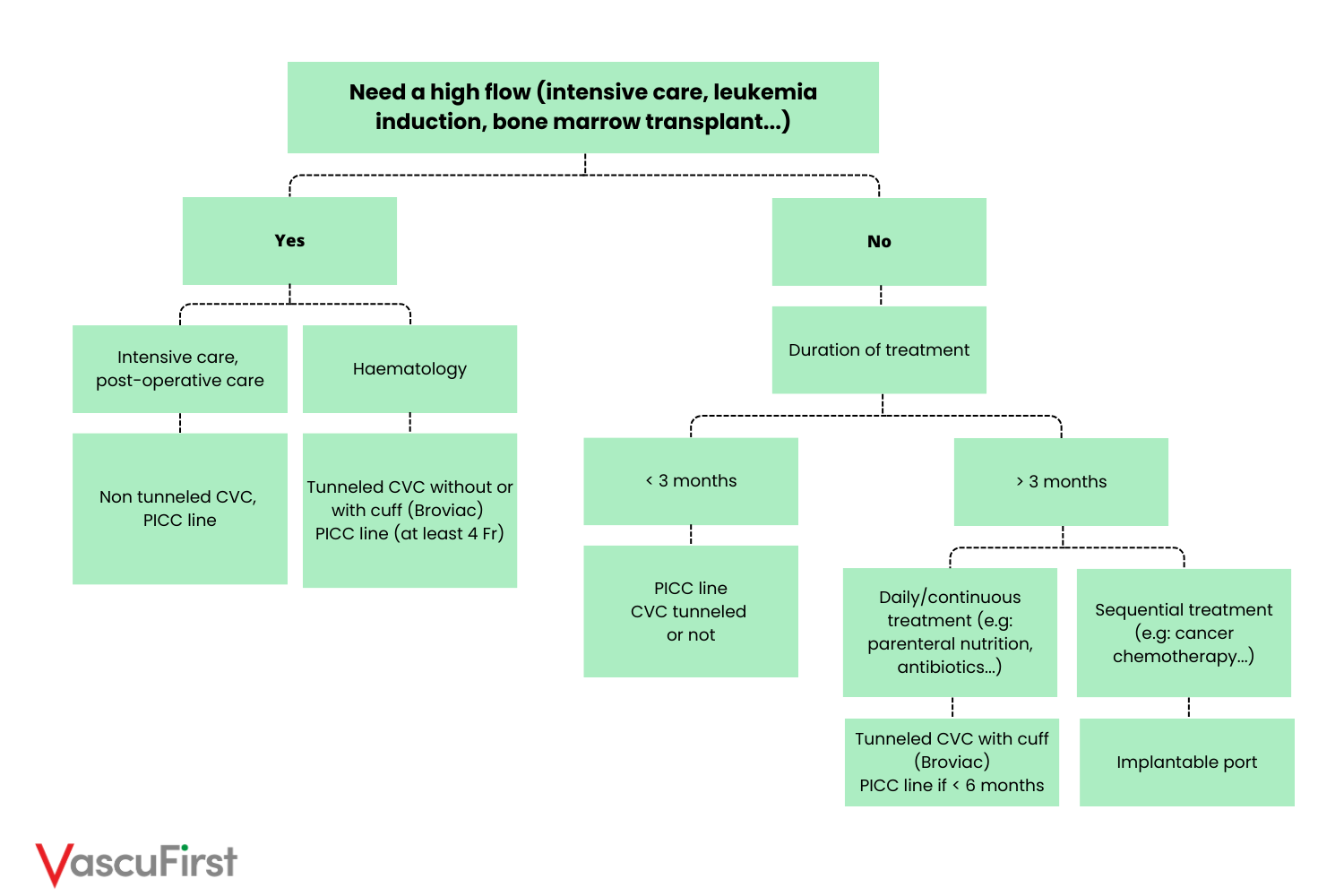
With small children, infants and newborns, meticulous attention should be given to device selection. In this perspective, the infographic below presents a decision tree for central venous device choice in pediatrics:
-
Device size choice
To select the appropriate catheter size for a child, you can refer to the chart below, which outlines size recommendations based on weight. This chart covers central venous catheters without cuff (CVCs), PICC lines, long-term catheters with cuff (Hickman-Broviac), and implantable ports.
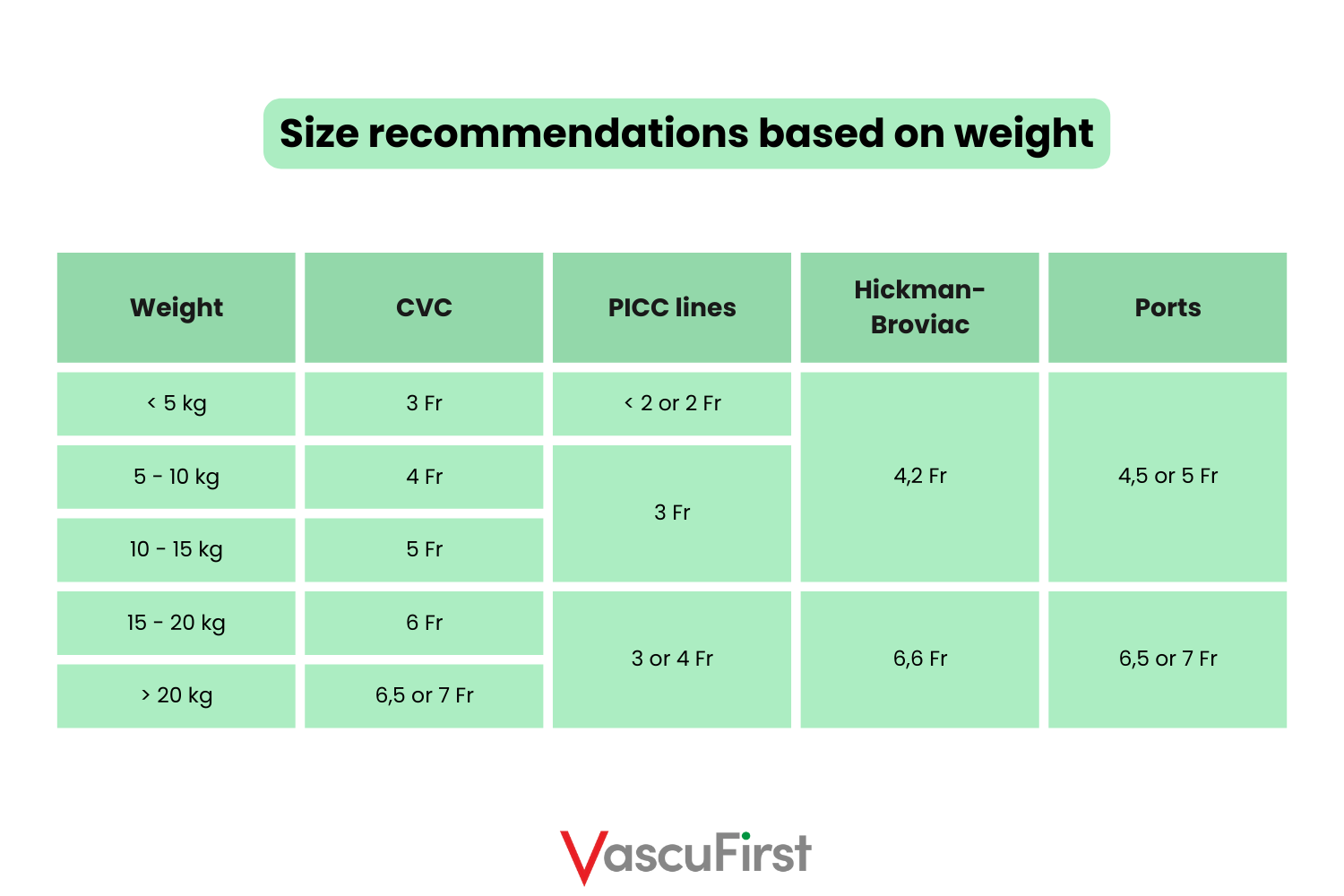
It is important to note that for multi-lumen CVCs, 1 Fr should be added to the recommended size indicated in the chart.
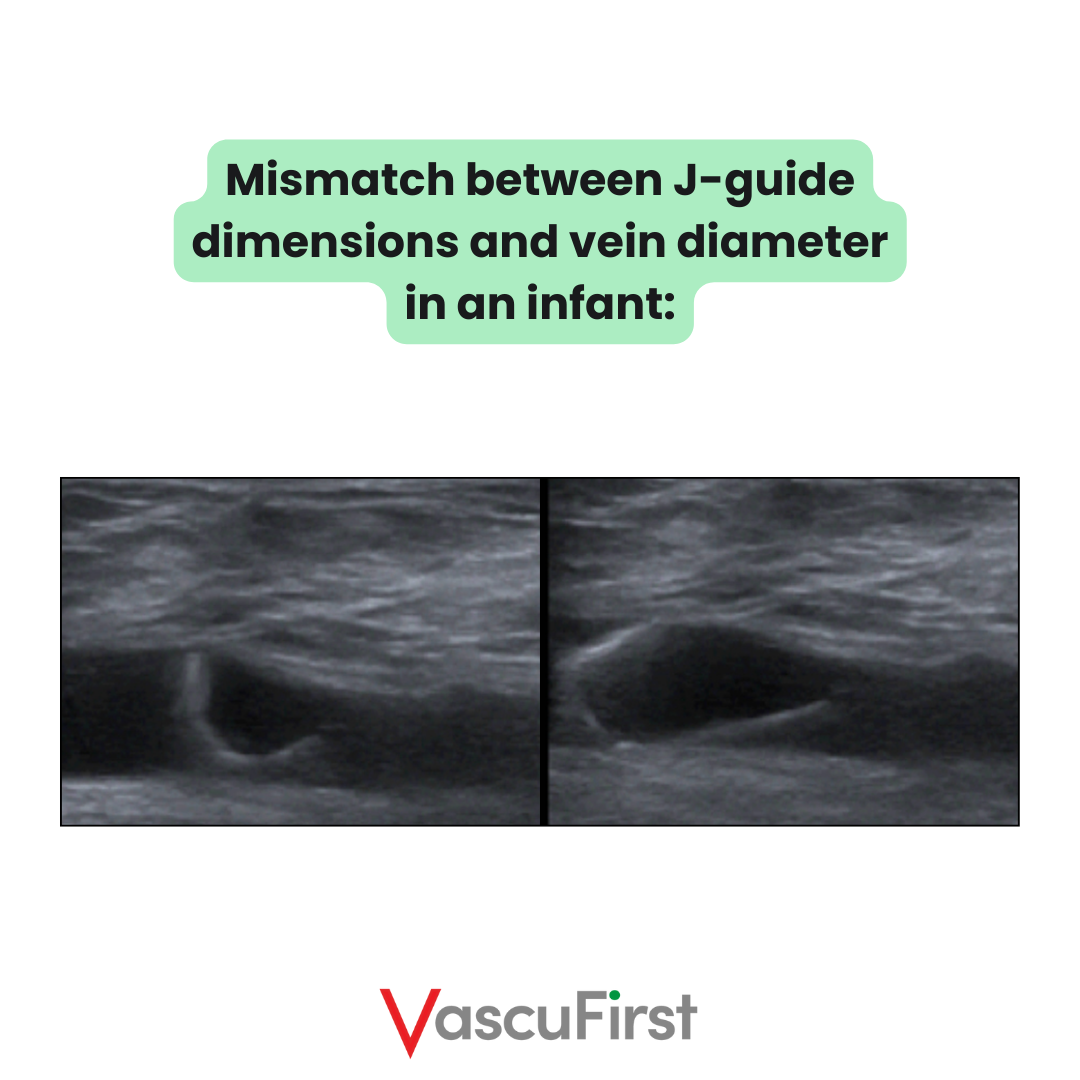
Additionally, exercise caution when using guidewires with infants. Given that the diameter of the jugular veins is almost of 5mm in 5kgs infants, the J guide is too wide for the veins, which impedes its progression. Therefore, it is recommended to use a straight wire with small infants.
• Choice of probe
Probe selection varies with the patient’s age:
– < 1 yr: hockey probe
– > 1 yr: normal linear probe is accurate.

• Positioning of the child (neck and thoracic approaches)
Head rotation should be limited for no more than 40 degrees. For newborns and infants, a small block should be placed under the shoulders to clear the neck. This technique is however not needed in older children and adults.

• Choice of vein (neck/thoracic approaches)
A group of French experts¹ has issued the following vein selection recommendations:
« An ultrasound-guided supraclavicular approach of the brachiocephalic vein should probably be preferred for central venous catheter insertion in infants and children, except in neonatology, to decrease the number of attempted cannulations and the immediate mechanical complications. »
These recommendations stem from the observation that internal jugular veins of infants and small children are excessively mobile and elastic, which increases the risk of transfixion and accidental carotid puncture. The risk of transfixing the internal jugular vein rises from around 15% in adults and children over 5 years to 50% in children aged 1 to 5 years and is close to 75% in newborns and infants < 1 year².
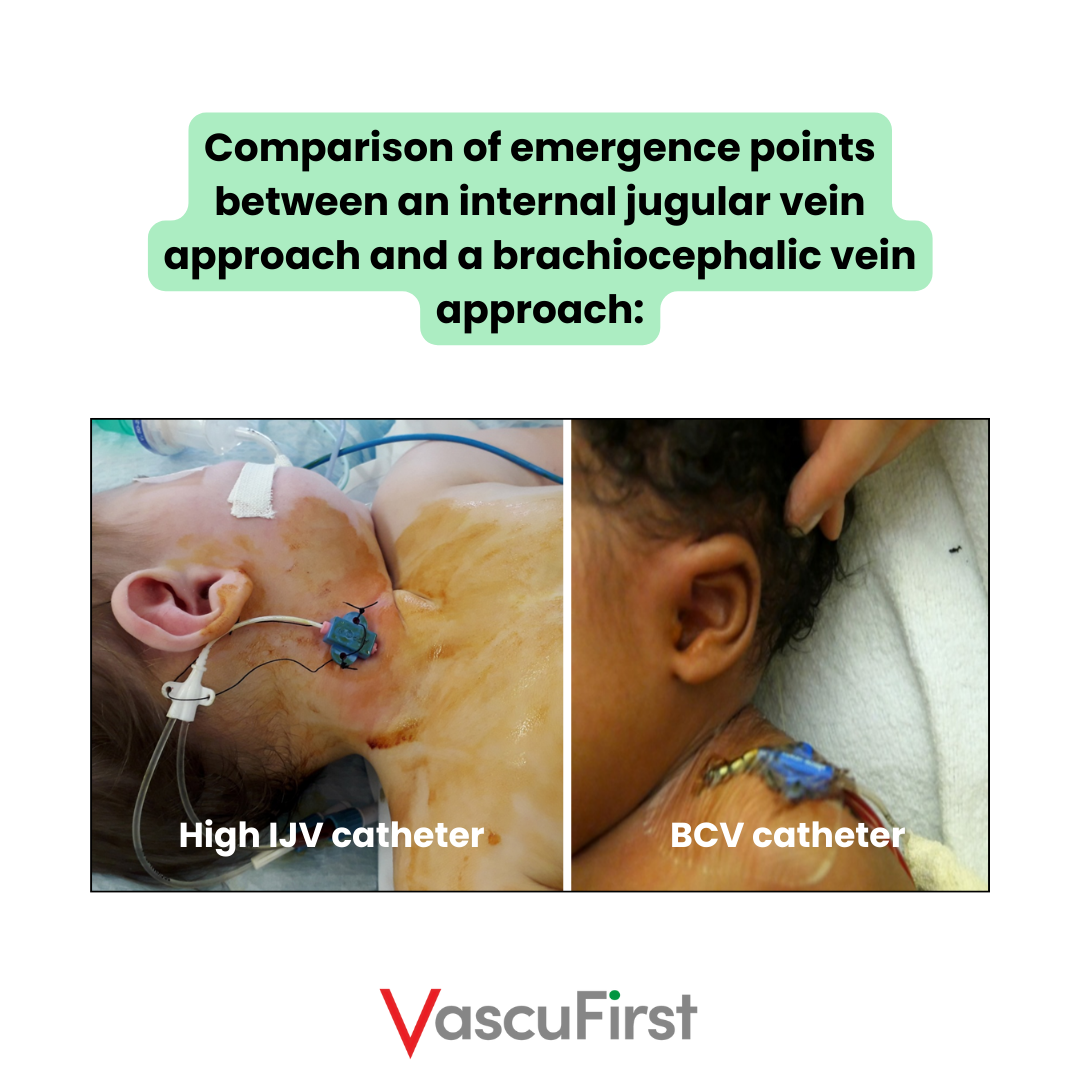
On the contrary, the brachiocephalic vein (jugulo-subclavian junction) is not mobile, and its diameter remains large even in hypovolemia. The puncture is performed under ultrasound guidance in plane and is aligned with the axis of the vein, so the guide advances very easily, with almost no risk of misdirection. This approach also allows the placement of relatively large catheters in very small infants³.

Finally, the supraclavicular approach to brachiocephalic veins makes dressing easier, more stable and more comfortable.
Conclusion:
Customizing the central venous access approach for small children, infants, and newborns is crucial for protecting their delicate veins. Practicians must carefully choose the appropriate central venous access device, size, ultrasound probe, and vein, while also ensuring accurate positioning of the child.
References:
– Timsit et al. Expert consensus-based clinical practice guidelines management of intravascular catheters in the intensive care unit. Ann Intensive Care. 2020; 10: 118.
– Tercan et al. Comparison of ultrasonography-guided central venous catheterization between adult and pediatric populations. Cardiovasc Intervent Radiology 2008; 31(3): 575-80
– Breschan et al. A Retrospective Analysis of the Clinical Effectiveness of Supraclavicular, Ultrasound-guided Brachiocephalic Vein Cannulations in Preterm Infants. Anesthesiology 2018; 128(1): 38-43


