Supporting Safe, Developmentally‑Appropriate Oral Feeding in Preterm Infants
For preterm and medically complex infants, transitioning from tube feeding to oral feeding is a highly individualised developmental journey. Enteral Feeding Guidelines emphasise a cue‑based, infant‑led approach, recognising that quality, safety, and positive experiences are more important than volume consumed. A structured, developmentally attuned transition helps prevent feeding complications, supports neurodevelopment, and strengthens parent–infant bonding.
This article outlines the readiness cues, techniques, tools, and protective strategies that neonatal teams can use to support safe and confident oral feeding.
1. Feeding Readiness Signs: The Foundation of Cue‑Based Feeding
According to guidelines, oral feeding should begin when the baby demonstrates readiness cues, not at a fixed gestational age or weight.
Key readiness indicators include:
- Stable physiological status (oxygenation, respiratory pattern, heart rate)
- Tolerance of full enteral feeds
- Ability to maintain alertness across the feeding period
- Organised behavioural state and engagement with care
- Demonstrated hunger cues such as rooting, bringing hands to mouth, or mouthing movements
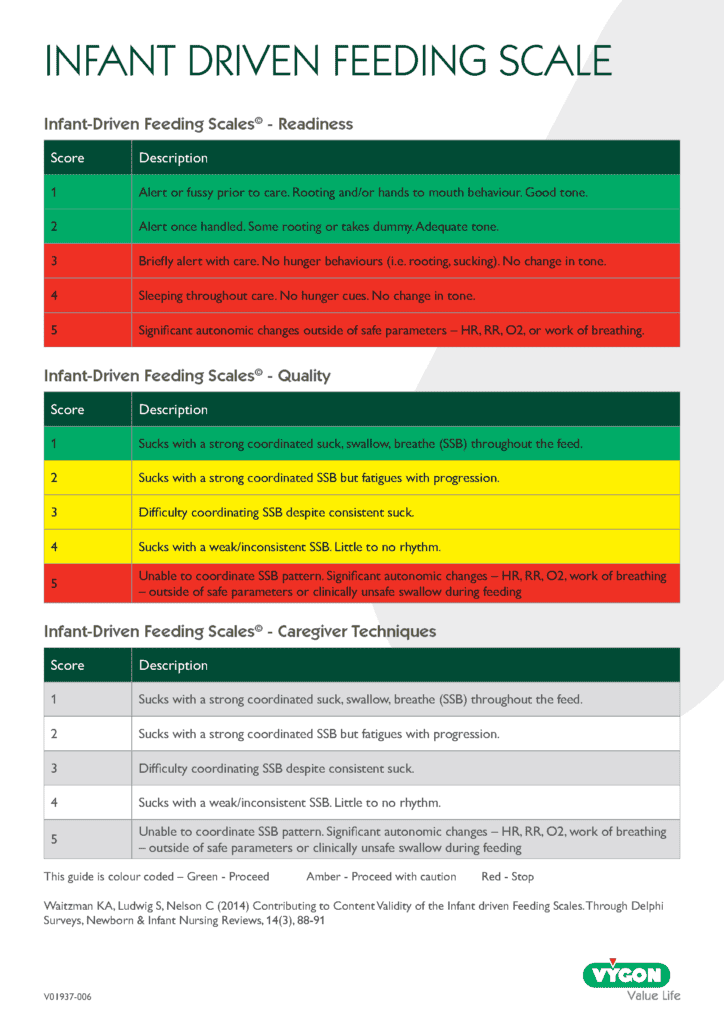
Recommendations are to use a consistent tool to measure readiness, such as the Infant‑Driven Feeding Scale (IDFS).
2. Supporting the Earliest Oral Feeds
Skilled Breastfeeding Techniques:
Breastfeeding is developmentally optimal for preterm infants, and several early practices can help support safe, successful progression to nutritive feeding.
Key strategies include:
- Providing skin‑to‑skin contact early and often to promote physiological stability and help infants become familiar with the breast environment.
- Encouraging non‑nutritive sucking (NNS) at the breast before formal breastfeeding begins, allowing infants to practise suck patterns without the expectation of milk transfer.
- Offering skilled positioning and attachment support from trained neonatal staff to help parents and infants establish effective early breastfeeding behaviours.
- Allowing infants to spend time at the breast even when milk transfer is minimal, reinforcing positive sensory experiences and supporting feeding confidence.
Rushing breastfeeding or relying on bottle feeding purely to accelerate discharge can create negative experiences and may disrupt feeding development. In the early stages, the quality of the feeding experience is more important than the quantity consumed, helping infants build safe, positive associations with oral feeding.
Skilled Bottle‑Feeding Techniques:
When bottle feeding is clinically appropriate or chosen by families, it is important to use a therapeutic, supportive approach that protects the infant’s developing oral skills.
Key techniques include:
- Elevated side‑lying positioning
- Ensuring use of an appropriate slow‑flow teat, as variable flow rates can overwhelm immature coordination patterns
- Avoiding prodding or “jiggling” the teat, which overrides infant cues and increases the risk of aspiration or feeding aversion
Parents should be thoroughly supported in these techniques and given time to understand their infant’s unique cues and pacing needs.
3. Positioning & Pace:
Positioning is essential to support suck–swallow–breathe coordination.
Elevated Side‑Lying Position
- Promotes physiological stability
- Supports airway protection
- Enhances the coordination of suck, swallow, and breathe
- Reduces choking episodes
- Improves feed volume tolerance
Side‑lying positioning facilitates safer bolus management and reduces desaturations, particularly in infants developing oral skills.
Supported Swaddling
Swaddling with hands toward the face provides postural stability and helps infants self‑regulate during oral feeds.
Pace Feeding
Many preterm infants have immature ability to independently pause during feeding. Pacing prevents apnoea, bradycardia, desaturations, and negative feeding experiences – benefits that extend into long‑term feeding success.
Key principles of pacing include:
- Removing or tipping the bottle to stop flow after several sucks
- Allowing the infant to breathe and re‑organise
- Watching for early signs of fatigue, stress, or desaturation
4. Preventing Oral Aversion: Protecting the Infant’s Emotional and Sensory Experience
Negative or forced feeding experiences can lead to long‑term oral aversion and feeding difficulties.
Strategies to prevent oral aversion include:
- Ensuring all oral feeding is infant‑led, not volume‑driven
- Avoiding forced pacing or excessive stimulation
- Using slow‑flow teats to prevent overwhelming flow
- Maintaining positive oral experiences earlier on (skin‑to‑skin, NNS, buccal colostrum)
- Stopping oral feeding attempts when the infant shows stress cues
- Ensuring consistency in techniques across caregivers and shifts
Cue‑based feeding protects the infant’s sense of safety and builds confidence in the feeding process.
Conclusion: A Developmentally Driven Journey
Transitioning from tube to oral feeding is not determined by age alone; it is a developmentally driven process shaped by physiological readiness, sensory maturation, meaningful family involvement, and skilled clinical support.
By using readiness cues, supportive positioning, pacing, and structured tools like the IDFS, neonatal teams can ensure that feeding becomes:
- Safe
- Positive
- Developmentally appropriate
- Emotionally protective
A place to learn about health procedures and techniques from leading professionals.
