Distinguishing Normal Immaturity from Early Warning Signs
Feed tolerance assessment is one of the most critical daily responsibilities in neonatal care. Preterm infants have immature gastrointestinal systems, making it challenging to distinguish normal adaptation from early signs of dysfunction or necrotising enterocolitis (NEC). A structured approach helps clinicians identify concerns promptly, reduce unnecessary interruptions to feeding, and protect infants from avoidable deterioration.
This article consolidates best‑practice principles to provide a practical, clinically usable framework for assessing feed tolerance, interpreting gastric residuals, evaluating aspirate colour, and differentiating intolerance from early NEC.
1. Understanding Feed Tolerance in Preterm Infants
Feed intolerance is common in preterm infants and often reflects the immaturity of gut motility rather than true pathology. Close monitoring is essential to avoid premature feed cessation -which can delay attainment of full enteral feeds-and to recognise genuine deterioration early.
Possible symptoms of feed intolerance include:
- Vomiting
- Gastric residuals >50% of the previous 4‑hour feed volume
- Abdominal distension
- Accompanying systemic symptoms (apnoea, bradycardia, poor perfusion, haemodynamic instability)
These signs require careful interpretation and correlation with the infant’s wider clinical picture.
2. Gastric Residual Volume (GRV) Guidance
The role of GRVs in assessing feed tolerance has evolved significantly.
Key principles:
- GRVs should only be checked every 4 hours until the infant is fully enterally fed or as per local policy. Routine checking is not recommended in stable infants on full feeds.
- Do not use GRV in isolation to stop or reduce feeds. GRVs are often elevated due to immaturity, medication effects, or positioning.
- Replace gastric residuals because they contain nutrients and enzymes that support intestinal maturation and motility.
- Small amounts of bile are not unusual in early feed establishment and should be interpreted carefully.
avoiding unnecessary feed interruptions- particularly because slower advancement prolongs the need for parenteral nutrition, increasing sepsis and catheter‑related risks.
Bile Aspirate Colour Assessment
Evaluating aspirate colour is essential to distinguishing normal variability from concerning pathology.
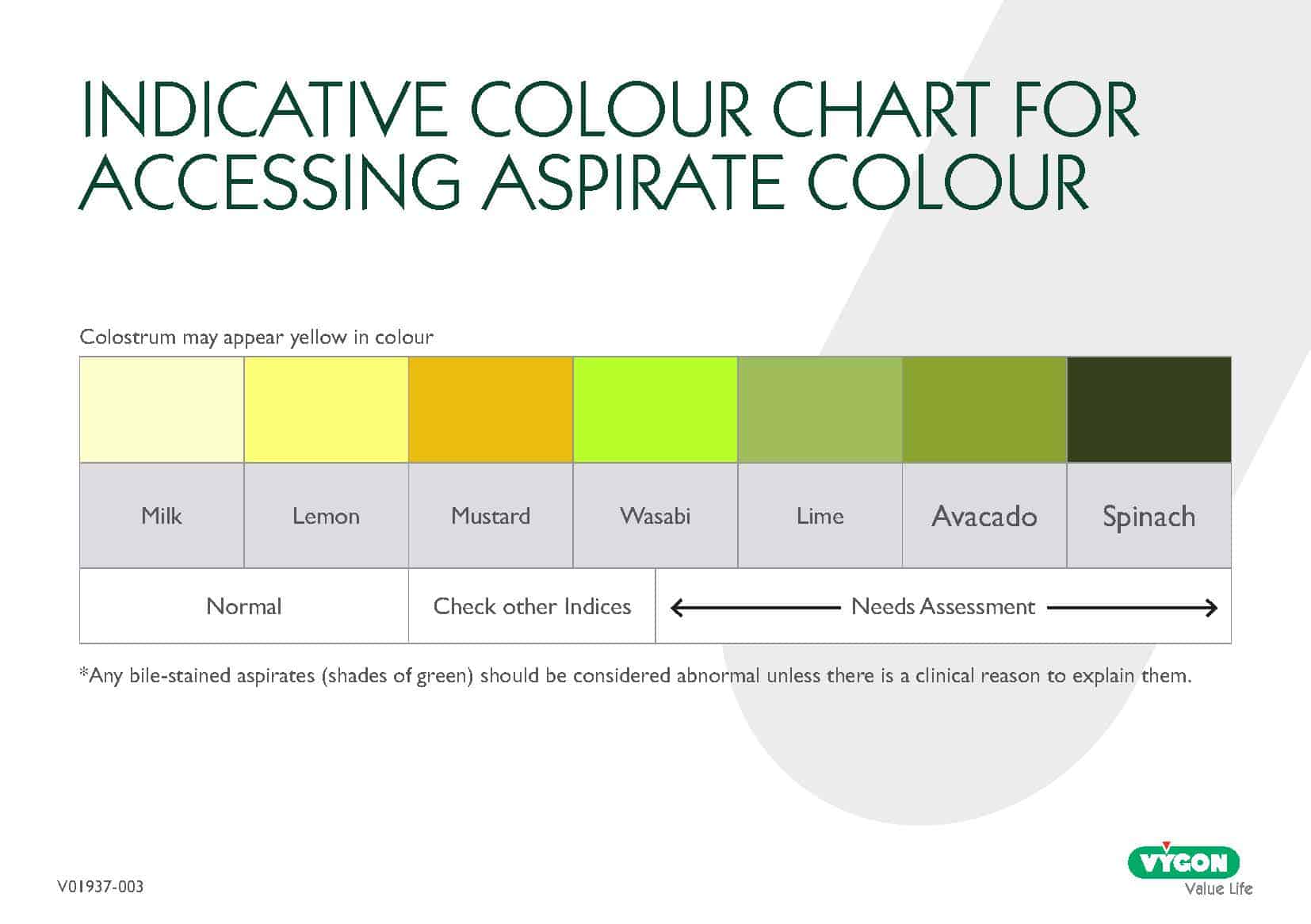
Normal or acceptable colours:
- Colostrum (yellow) is normal and expected.
- Pale or slightly milky residuals are also common during feed establishment.
Colours requiring assessment:
- Bile‑stained aspirates (green shades) should generally be considered abnormal unless a clear clinical explanation exists.
Action steps when colour is abnormal:
- Perform a full clinical review
- Consider septic screening according to local policy
- Assess for additional symptoms of intolerance or NEC
- If NEC is excluded, continuing trophic feeds may be preferable to stopping feeds entirely
This structured interpretation helps clinicians avoid both over‑reacting and under‑reacting to colour changes.
3. Differentiating Feed Intolerance from Early NEC
Because early NEC and feed intolerance can present similarly, differentiation must be systematic.
Possible symptoms of early NEC:
- Bilious or bloody aspirates
- Abdominal discolouration or visible bowel loops
- Bloody or watery stools
- Systemic deterioration (temperature instability, apnoea, lethargy, hypotension)
Key differentiators:
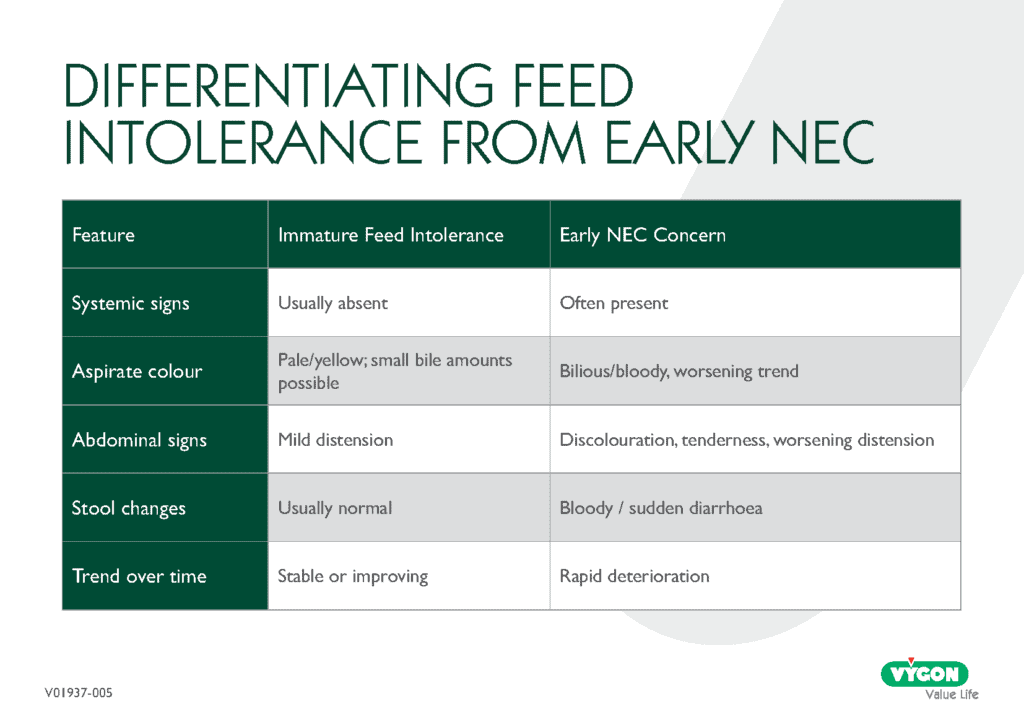
When in doubt, early escalation and surgical referral pathways are appropriate.
4. Practical Decision Tools for Daily Use
Daily Feeding Assessment Checklist
- Review GRV (if indicated) and replace residuals
- Assess aspirate colour against the colour chart
- Check abdominal shape and girth
- Evaluate systemic wellbeing (HR, RR, perfusion, temperature)
- Correlate findings with recent feeding progression
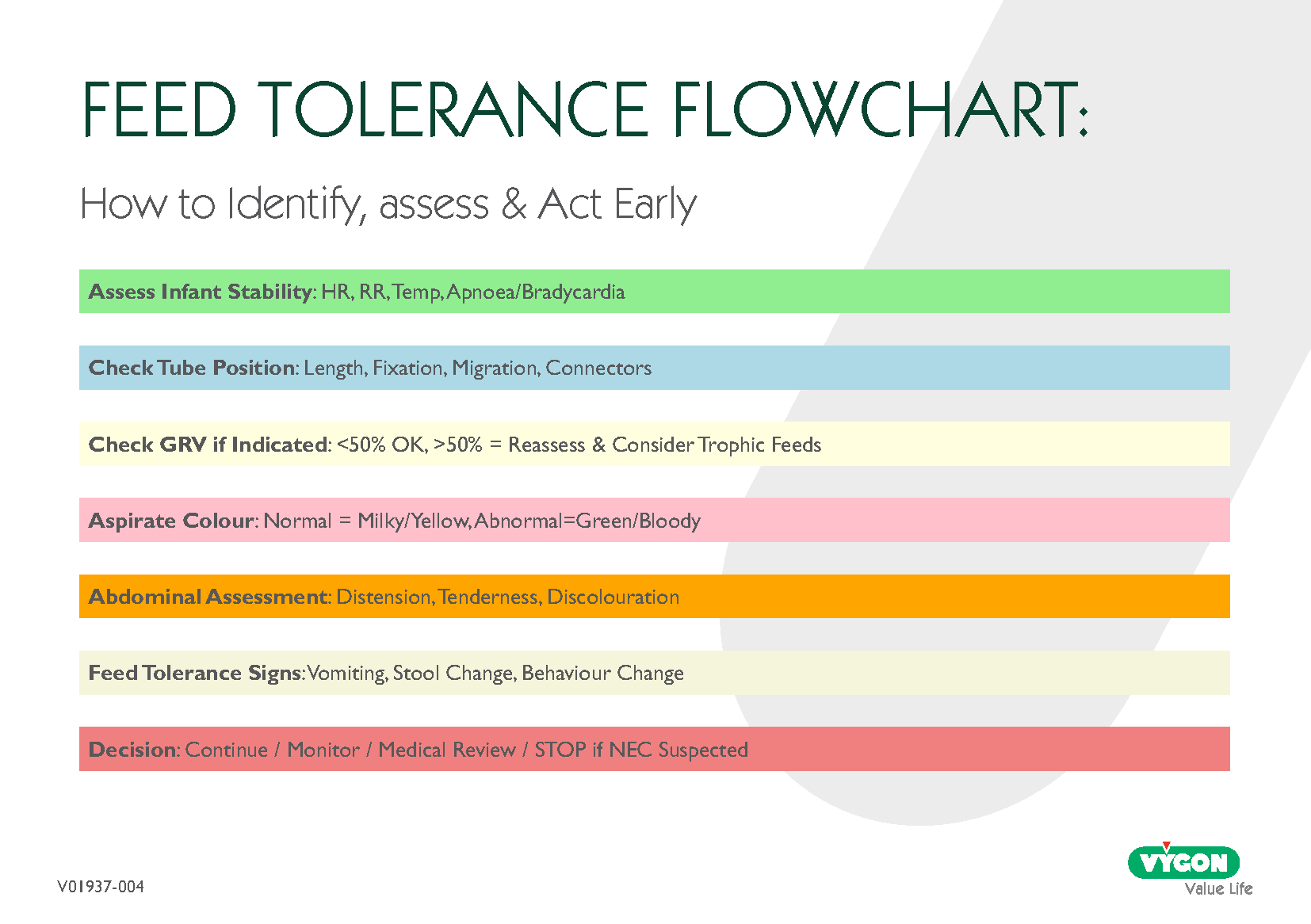
Assessment next steps
- Reassuring findings:
→ Continue feeds / advance per plan - Mild intolerance without systemic signs:
→ Consider maintaining trophic feeds, reassess frequently - Concerning colour or increasing GRV plus symptoms:
→ Medical review, consider septic screen - Signs consistent with possible NEC:
→ Stop feeds, follow NEC referral pathway
This approach aligns with recommendations to maintain enteral stimulation where safe, while act decisively when NEC is suspected.
Conclusion
Early, structured identification of feed tolerance helps protect infants from both underfeeding and avoidable harm. By applying consistent GRV assessment, colour interpretation, and differentiation between intolerance and early NEC, clinicians can support safer feeding progression while reducing unnecessary interruptions.
Next article:

Transitioning from Tube to Oral Feeding: A Cue‑Based Approach
A place to learn about health procedures and techniques from leading professionals.
